Explore comprehensive co-occurring disorder care strategies that improve addiction treatment outcomes and support lasting recovery.

Having both an addiction and a mental health condition at the same time makes recovery harder. Most treatment programs focus on one problem or the other, which is why they fail so often.
At Addiction Resource Center, we believe co-occurring disorder care requires treating both conditions together. This introduction explains why integrated treatment works better and how we approach dual diagnosis recovery.
Understanding Co-Occurring Disorders: Definition, Prevalence, and Why They Matter
Co-occurring disorders happen when someone has both a substance use disorder and a mental health condition at the same time. According to SAMHSA’s 2024 National Survey on Drug Use and Health, about 21.2 million adults in the United States have co-occurring mental illness and a substance use disorder. This isn’t rare or unusual-it’s the norm for a significant portion of people struggling with addiction. The most common mental health conditions paired with addiction include anxiety disorders, depression, PTSD, bipolar disorder, and ADHD.
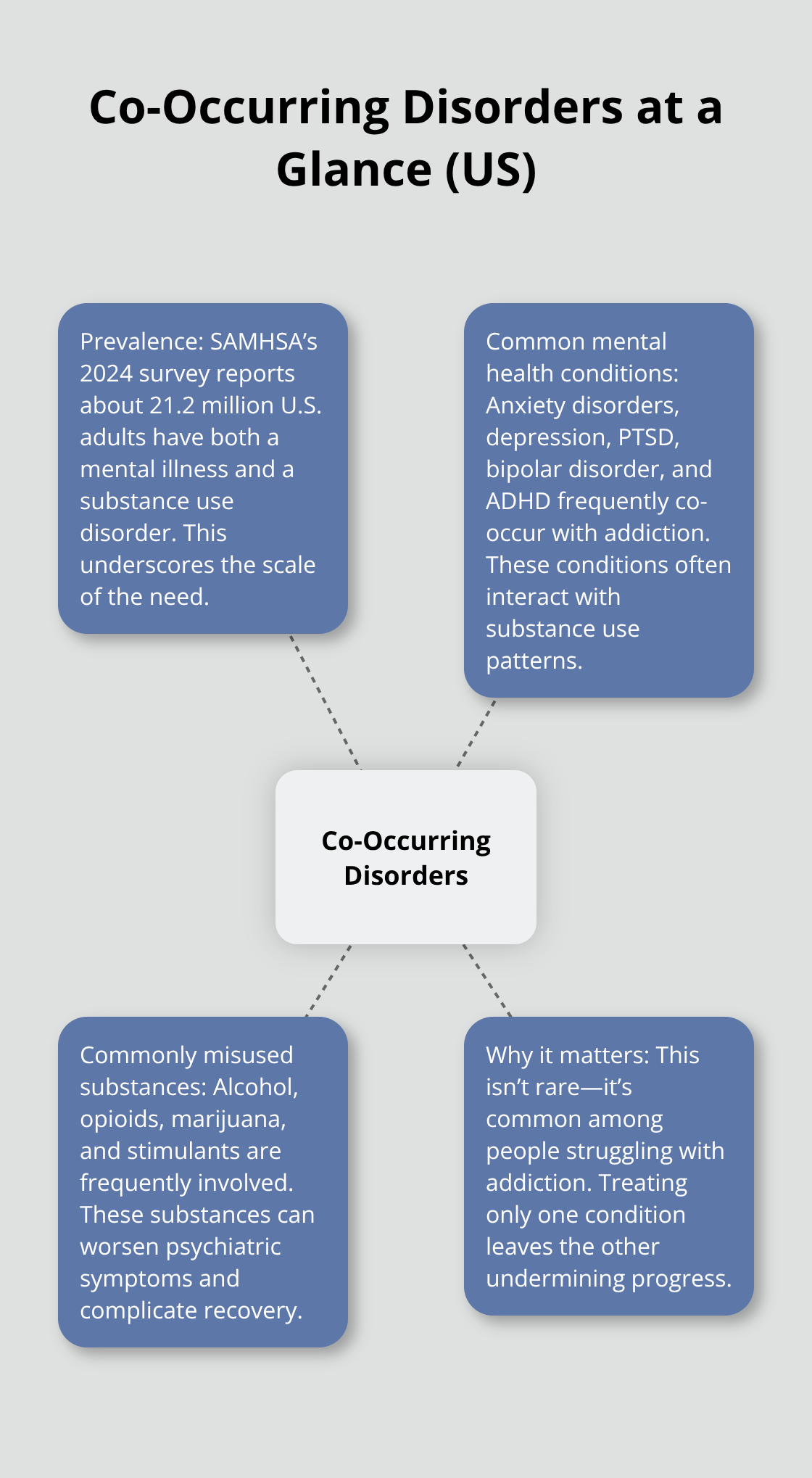
Alcohol, opioids, marijuana, and stimulants are frequently misused by people with these dual diagnoses.
How Co-Occurring Disorders Amplify Each Other
When both conditions exist together, they make each other worse. Someone with depression who drinks heavily experiences deeper depressive episodes. Someone with anxiety who uses stimulants faces intensified panic and paranoia. The brain systems involved in mood, anxiety, and addiction overlap significantly (dopamine pathways, serotonin regulation, and endocannabinoid systems all interact), which means treating only one condition leaves the other untreated and actively undermining recovery. This neurological overlap explains why people with co-occurring disorders show higher symptom severity and more complicated treatment paths than those with single diagnoses.
Why Fragmented Treatment Fails
Traditional addiction treatment programs ask about mental health history but don’t integrate treatment for it. Similarly, mental health clinics screen for substance use but refer clients elsewhere for addiction care. This separation is catastrophic for people with co-occurring disorders. Research consistently shows that integrated treatment produces significantly better outcomes than sequential or parallel treatment. Someone attending a mental health clinic on Tuesday and an addiction program on Thursday experiences fragmented care, conflicting advice, and medication interactions that nobody monitors. Dropout rates climb higher because clients don’t see how their treatment addresses their complete reality.
The Real-World Impact on Recovery Outcomes
When co-occurring disorders go untreated as a combined issue, relapse rates spike dramatically. Research shows that people receiving integrated care have better housing stability, fewer hospitalizations, and lower arrest rates compared to those in single-focus programs. The cost difference matters too-fragmented care leads to emergency room visits, crisis interventions, and repeated treatment cycles that drain both personal resources and healthcare systems. Someone with opioid use disorder and depression needs medication-assisted treatment paired with antidepressants and therapy that addresses both conditions together, not separate prescriptions from different providers who don’t communicate. The timing of treatment also matters; early intervention before conditions become severe yields better long-term outcomes than waiting until someone reaches crisis point.
What Integrated Care Looks Like
Integrated treatment combines addiction services with mental health services delivered by the same multidisciplinary team. This approach uses pharmacological interventions (medications), psychological therapies, and behavioral strategies that target both conditions simultaneously. Treatment teams include addiction specialists, mental health clinicians, and case managers who coordinate care and monitor for medication interactions. The model emphasizes individualized assessment, which means clinicians identify the specific combination of disorders each person has rather than applying a one-size-fits-all approach. This comprehensive strategy addresses the overlapping brain systems and life circumstances that fuel both addiction and mental health conditions, setting the stage for sustainable recovery.
Medication and Therapy Work Together in Dual Diagnosis Treatment
Integrated Medication Management Prevents Dangerous Interactions
Treating addiction and mental health simultaneously requires medications that address both conditions without creating dangerous interactions. Medication-assisted treatment (MAT) forms the backbone of effective dual diagnosis care. For opioid use disorder paired with depression, buprenorphine or methadone tackles cravings while antidepressants stabilize mood. For alcohol use disorder with anxiety, naltrexone reduces drinking urges while SSRIs address anxiety symptoms.
The critical mistake occurs when clinicians prescribe benzodiazepines like Xanax or Valium alongside MAT medications. This combination causes serious adverse effects, including overdose risk. SAMHSA’s treatment guidelines explicitly warn against this pairing.

Acamprosate and disulfiram offer safer alternatives for alcohol use disorder when benzodiazepines seem tempting but dangerous.
One treatment team that monitors all medications together catches interactions before they harm the client and adjusts prescriptions based on how both conditions respond. Research from multiple addiction medicine studies confirms that integrated medication management produces better abstinence rates and symptom improvement than separate prescribing from different providers.
Trauma-Informed Therapy Addresses Root Causes
Therapy without trauma awareness fails most people in dual diagnosis care. Trauma histories drive both addiction and mental health conditions in the majority of cases. Trauma-informed care means clinicians understand how past abuse, neglect, or violence shaped current symptoms and substance use patterns.
This approach avoids retraumatization during treatment, which happens frequently when therapists push clients to discuss trauma before stabilization occurs. The correct sequence starts with behavioral stabilization, crisis management, and safety planning before trauma processing begins. Cognitive behavioral therapy works well for dual diagnosis when therapists integrate trauma-informed principles and address how trauma cues trigger both substance use and mental health symptoms.
For someone with PTSD and opioid use disorder, exposure-based trauma therapy must happen after the person achieves stable housing, medication compliance, and reduced substance use. Attempting it earlier guarantees dropout and relapse.
Building Engagement Through Motivational Approaches
Motivational interviewing paired with contingency management addresses the resistance and ambivalence that plague dual diagnosis clients. The therapist’s job involves reducing emotional reactivity in sessions, coordinating with case managers and peer support networks, and recognizing that recovery happens in small increments, not dramatic breakthroughs.
Treatment should be time-unlimited with assertive outreach because dual diagnosis clients drop out more frequently than single-diagnosis populations. Programs that pursue clients after missed appointments and adjust treatment based on real-world obstacles see dramatically higher engagement and success rates. This persistence transforms outcomes for people who struggle with both addiction and mental health conditions simultaneously.
How We Treat Co-Occurring Disorders
Assessment That Identifies Both Conditions Together
Effective co-occurring disorder treatment starts with assessment that identifies both the addiction and the mental health condition simultaneously, not sequentially. Many programs screen for mental health after addiction assessment concludes, which means clinicians miss critical diagnostic details that shape the entire treatment plan. Integrated assessments evaluate substance use patterns, mental health symptoms, trauma history, medication interactions, and social stability in one comprehensive process. This approach takes longer upfront but prevents the costly mistakes that occur when clinicians treat depression without understanding that alcohol use represents self-medication for mood symptoms, or when they address anxiety without recognizing that stimulant use amplifies panic.
Assessment identifies the specific neurobiological overlap in each client’s situation. Someone with opioid use disorder and depression has different brain chemistry than someone with alcohol use disorder and PTSD, so their medication and therapy combinations differ significantly. Screening also covers co-occurring health conditions like chronic pain, HIV risk, and hepatitis exposure because these conditions intersect with both addiction and mental health treatment decisions. Validated screening tools help clinicians catch diagnoses that clients themselves don’t recognize as separate problems.
Coordinated Teams Prevent Medication Interactions
A multidisciplinary team model means addiction specialists, mental health clinicians, psychiatric nurses, and case managers work together in the same organization with shared client records and coordinated treatment plans. This integration prevents the dangerous medication interactions that occur when different providers prescribe without communication. If a psychiatrist prescribes an SSRI for depression and an addiction medicine doctor prescribes buprenorphine for opioid use disorder, a coordinated team monitors how these medications interact and adjusts dosing based on real treatment response.

Research consistently demonstrates that integrated teams reduce relapse rates, hospitalizations, and arrests compared to fragmented care models. One treatment organization that monitors all medications together catches interactions before they harm the client and adjusts prescriptions based on how both conditions respond.
Evidence-Based Therapies for Dual Diagnosis
Treatment uses evidence-based therapies including cognitive behavioral therapy adapted for trauma-informed dual diagnosis work, motivational interviewing to address ambivalence about recovery, and contingency management that reinforces both abstinence and mental health symptom improvement. Trauma-informed therapy addresses root causes because trauma histories drive both addiction and mental health conditions. This approach avoids retraumatization during treatment, which occurs frequently when therapists push clients to discuss trauma before stabilization happens.
The correct sequence starts with behavioral stabilization, crisis management, and safety planning before trauma processing begins. For someone with PTSD and opioid use disorder, exposure-based trauma therapy must happen after the person achieves stable housing, medication compliance, and reduced substance use.
Sustained Engagement and Practical Support
Treatment remains time-unlimited with assertive outreach because dual diagnosis clients drop out more frequently than single-diagnosis populations. Treatment teams pursue engagement after missed appointments rather than discharging clients. Employment support and stable housing assistance integrate into treatment because housing instability and unemployment dramatically increase relapse risk in this population. Motivational interviewing paired with contingency management addresses the resistance and ambivalence that plague dual diagnosis clients. The therapist’s role involves reducing emotional reactivity in sessions, coordinating with case managers and peer support networks, and recognizing that recovery happens in small increments, not dramatic breakthroughs.
Final Thoughts
Co-occurring disorder care works because it treats the whole person, not isolated symptoms. Integrated treatment produces better housing stability, fewer hospitalizations, and lower relapse rates than fragmented approaches. When addiction and mental health conditions are addressed together by coordinated teams using evidence-based therapies and medication management, people recover at higher rates and stay engaged longer.
Someone with depression and alcohol use disorder needs both antidepressants and naltrexone managed by providers who communicate with each other. Someone with PTSD and opioid use disorder needs trauma-informed therapy paired with buprenorphine, delivered by a team that monitors medication interactions and adjusts treatment based on real progress. Separate appointments at different clinics guarantee failure, while integrated care delivered by multidisciplinary teams guarantees better outcomes.
If you or someone you know struggles with both addiction and mental health conditions, comprehensive co-occurring disorder care is available. We at Addiction Resource Center in Yuba City provide personalized addiction therapy and mental health support designed specifically for dual diagnosis. Our multidisciplinary team conducts integrated assessments, manages medications safely, and delivers evidence-based therapies that address both conditions together.