Understand dual diagnosis and addiction: learn how co-occurring mental health and substance use disorders interact, plus treatment strategies that work.

Roughly 9 million American adults struggle with both addiction and mental health disorders simultaneously. When these conditions occur together, treating one without addressing the other typically leads to relapse and continued suffering.
At Addiction Resource Center, we’ve seen firsthand how dual diagnosis and addiction require a completely different treatment approach than single-condition recovery. This guide walks you through what dual diagnosis actually means, why standard treatment fails, and how integrated care changes outcomes.
What Dual Diagnosis Really Looks Like
The Feedback Loop Between Mental Illness and Substance Use
Dual diagnosis means a person has both a substance use disorder and a mental health condition at the same time, and these two conditions actively fuel each other. It is not simply having two separate problems that happen to exist in one person. The National Institute on Drug Abuse reports that roughly half of people with a mental illness will experience a substance use disorder at some point in their lives, and this relationship runs both directions. When someone has untreated depression, they turn to alcohol to manage the emotional weight. When someone uses stimulants regularly, those drugs trigger or worsen anxiety disorders and paranoia. The feedback loop between mental illness and substance use creates a self-perpetuating cycle where each condition makes the other worse, which is exactly why treating only one condition fails so dramatically.
Someone might stop drinking but remain trapped in severe anxiety, leading them straight back to the bottle. Another person might stabilize their bipolar symptoms with medication but continue using cocaine, which destabilizes their mood all over again. This gap matters because it means many people spend years struggling with untreated mental health symptoms before they ever touch drugs or alcohol, making them vulnerable targets for self-medication.
How Common Dual Diagnosis Actually Is
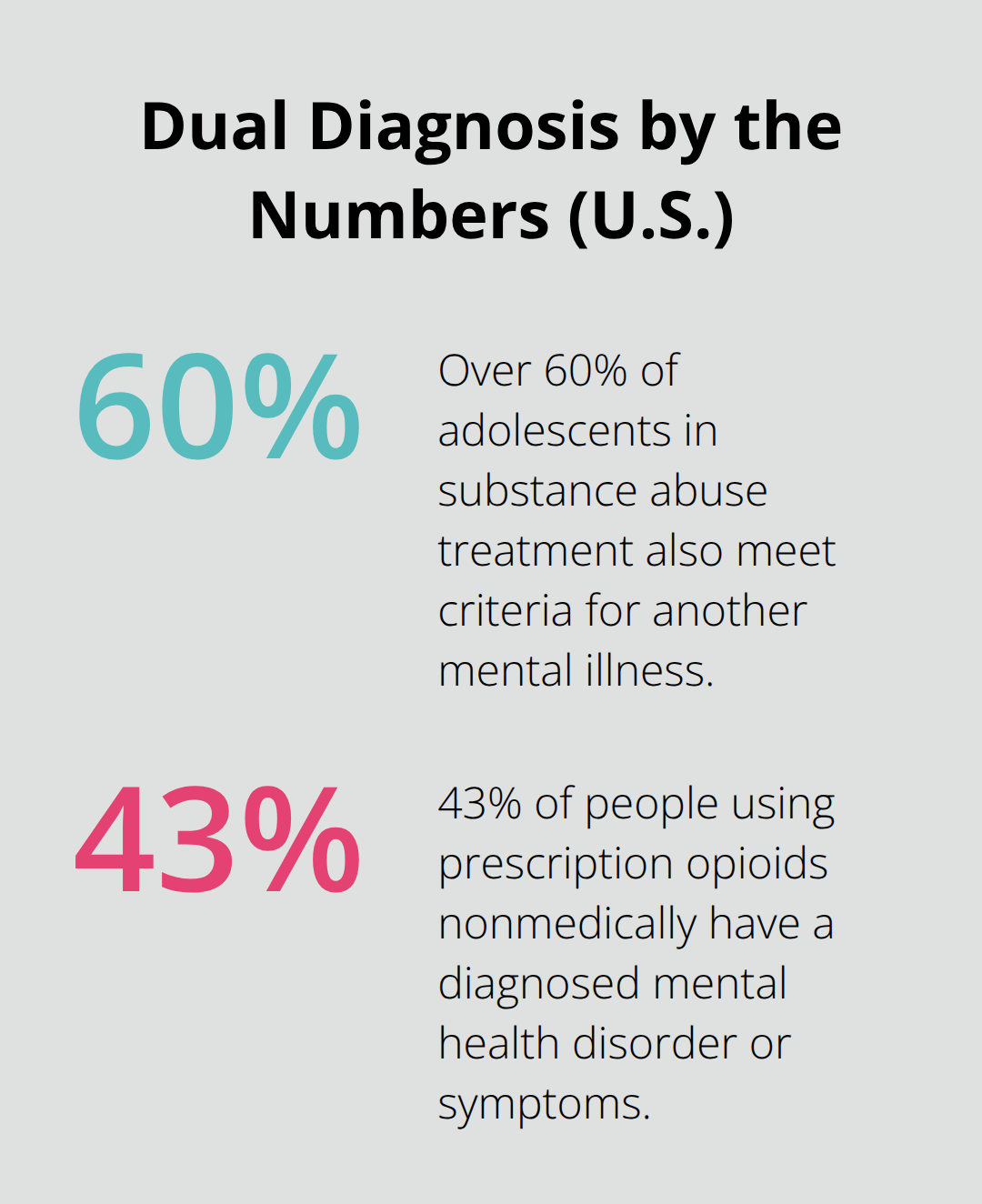
The statistics on dual diagnosis demand attention from anyone in recovery. About 10 million American adults experience both conditions in any given year. Among people in substance abuse treatment specifically, over 60 percent of adolescents and a significant percentage of adults also meet criteria for another mental illness. The National Institute on Drug Abuse notes that among people using prescription opioids nonmedically, 43 percent have a diagnosed mental health disorder or symptoms.
Depression and anxiety are the most common co-occurring conditions, but dual diagnosis also appears alongside bipolar disorder, ADHD, psychotic illnesses, and personality disorders.
High-risk populations show even higher rates. About 1 in 5 veterans with PTSD also has a co-occurring substance use disorder. People experiencing homelessness have dual disorders at rates between 10 and 20 percent. The prison population includes more than 1 million individuals with both mental illness and substance use disorders. These numbers reveal that dual diagnosis is not rare or exceptional-it is the norm for many people in treatment.
Why Integrated Treatment Works Better
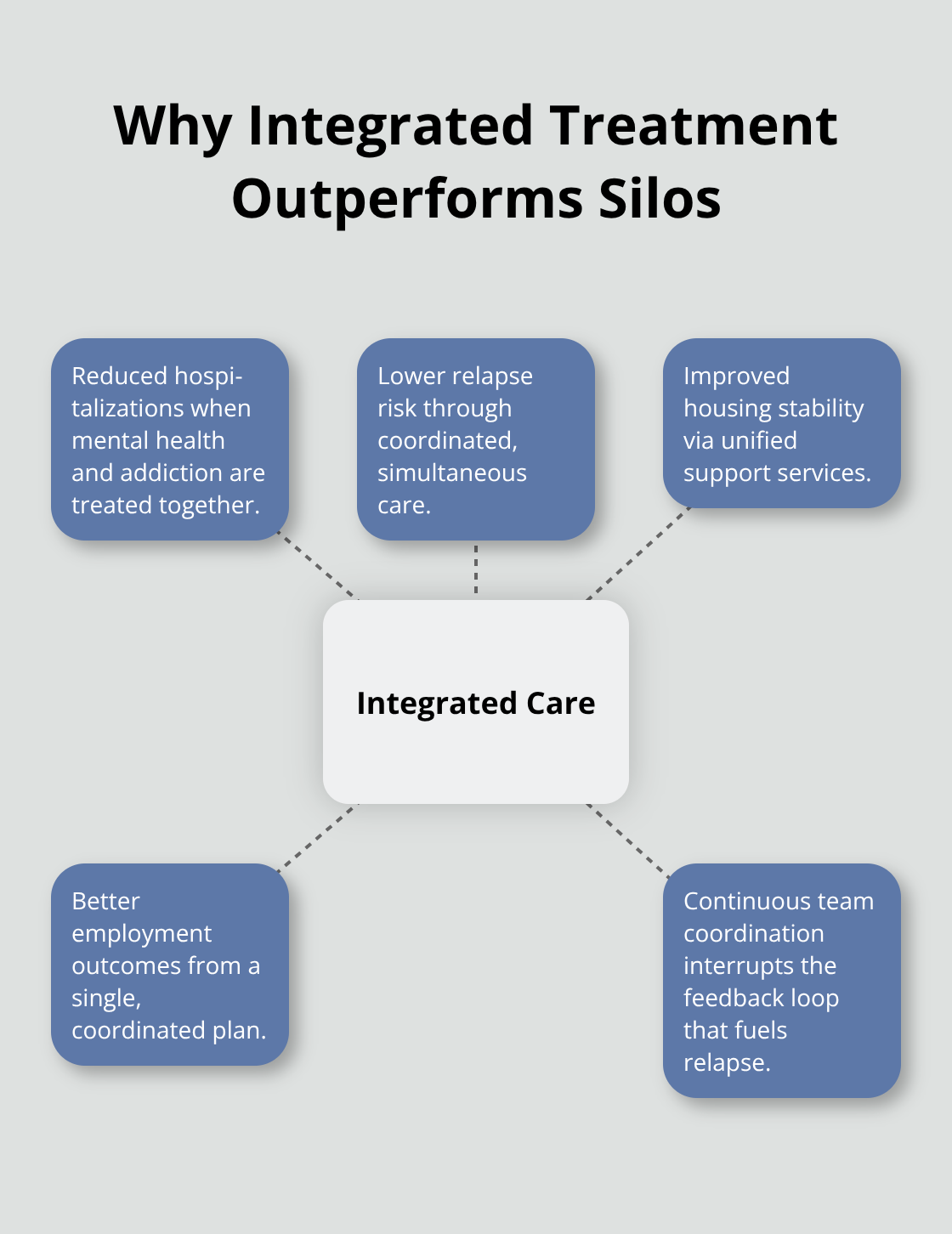
What makes these statistics actionable rather than just alarming is understanding that integrated treatment addresses both conditions simultaneously and produces measurably better outcomes than treating them separately. This is not a suggestion or a preference. The evidence shows reduced hospitalization rates, lower relapse risk, improved housing stability, and better employment outcomes when both disorders receive coordinated care from the same treatment team. When clinicians treat mental health and addiction together (rather than in separate silos), they interrupt the feedback loop that keeps people trapped in cycles of relapse and crisis.
The next section explores the specific treatment models that make this integrated approach work and how they differ fundamentally from traditional single-condition recovery programs.
How Dual Diagnosis Treatment Actually Works
Integrated Dual Disorder Treatment, or IDDT, stands as the gold standard for dual diagnosis because it treats mental health and substance use in the same setting with coordinated teams rather than sending people between separate providers. This matters enormously because the feedback loop between conditions means progress in one area directly impacts the other. IDDT applies a stage-of-change approach, delivering small overlapping changes over time so people stabilize their moods and manage cravings simultaneously rather than chasing one goal while the other deteriorates. The model combines medication management, individual and group counseling, family education, supported employment, and housing support into one coherent plan. Research shows IDDT reduces relapse, hospitalization, and arrests while improving quality of life and employment outcomes. The Dartmouth Psychiatric Research Center developed this framework decades ago, and SAMHSA now guides national implementation.
Most critically, IDDT keeps people engaged long-term because the treatment team understands that someone with bipolar disorder and cocaine addiction cannot simply stop using drugs and hope their mood stabilizes on its own. The two conditions require simultaneous attention from clinicians trained in both mental health and addiction medicine.
Medication and Counseling Address Biology and Psychology Together
Medication-assisted therapy paired with counseling addresses the biological and psychological sides of dual diagnosis at once. For someone with depression and alcohol dependence, an antidepressant reduces the emotional pain that drives drinking while therapy teaches coping skills for managing cravings and triggers. For opioid use disorder with anxiety, medications like buprenorphine stabilize brain chemistry while cognitive behavioral therapy rewires thought patterns that fuel both addiction and panic. The National Institute on Drug Abuse confirms that this combination approach works better than either treatment alone. Clinicians must select medications carefully because some drugs interact dangerously with substances or worsen psychiatric symptoms. Bupropion treats depression while reducing nicotine cravings, making it valuable for people struggling with both. Naltrexone blocks opioid effects while also reducing alcohol cravings. Medication management requires ongoing adjustment because substance use itself changes brain chemistry, and as people stop using drugs or alcohol, their psychiatric symptoms often shift. Weekly or biweekly appointments ensure medications stay effective and side effects receive attention before they derail recovery.
Specialists Recognize What General Practitioners Miss
Dual diagnosis specialists understand that standard addiction or mental health treatment protocols fail for this population. A therapist trained only in addiction treatment might push someone to stop drinking immediately while missing that their client’s bipolar disorder makes impulsive decisions harder to control. A psychiatrist focused solely on mental health might prescribe medications without asking about substance use patterns that could interact dangerously or worsen addiction. Specialists screen for both conditions simultaneously, adjust treatment plans when progress stalls, and recognize that relapse often signals either an unaddressed psychiatric symptom or a medication that needs changing rather than personal failure. They know that people with dual diagnosis need longer treatment timelines and more frequent contact than single-condition populations. They understand that housing and employment stability directly impact recovery outcomes, so they coordinate with social services rather than treating addiction in isolation. Finding clinicians with this dual expertise remains difficult across most regions, but treatment programs specifically designed for dual diagnosis employ multidisciplinary teams (psychiatrists, addiction counselors, therapists, and case managers) working from the same treatment plan.
How Treatment Teams Prevent the Relapse Cycle
When mental health and addiction treatment operate separately, people fall through gaps that lead directly back to substance use. A client stabilizes their depression with medication but continues using stimulants, which destabilizes their mood again. Another person stops drinking but faces untreated anxiety that becomes unbearable within weeks. Integrated teams prevent this pattern because they monitor both conditions constantly and adjust interventions when one area threatens the other. If someone’s psychiatric symptoms worsen, the team increases therapy sessions or modifies medication rather than assuming the person lacks motivation. If cravings spike, clinicians investigate whether an underlying mental health symptom (like insomnia or irritability) triggered the urge to use. This coordinated approach means treatment addresses the actual problem instead of treating symptoms in isolation. The team also maintains contact over months and years rather than discharging people after a fixed program length, which matters because dual diagnosis recovery follows a longer timeline than single-condition treatment.
The next section examines the specific barriers that prevent people from accessing this integrated care and how those obstacles shape recovery outcomes across different populations.
Why Single-Disorder Treatment Fails with Dual Diagnosis
Traditional addiction programs treat substance use as the primary problem and expect mental health symptoms to resolve once someone stops using drugs or alcohol. This approach fails catastrophically for people with dual diagnosis because their psychiatric conditions exist independently and demand their own treatment. Someone with depression does not suddenly feel better after 30 days sober; the depression persists and intensifies, driving them straight back to alcohol as a coping mechanism. A person with untreated anxiety cannot simply will away panic attacks through abstinence alone. The National Institute on Drug Abuse reports that among people in treatment for nonmedical prescription opioid use, 43 percent have a diagnosed mental health disorder, yet most programs focus exclusively on stopping the drug use. Similarly, mental health clinics that ignore substance use miss the fact that someone’s cocaine use destabilizes their bipolar disorder or that their drinking masks underlying PTSD symptoms. This siloed approach creates a dangerous situation where people complete treatment programs feeling worse than when they arrived because one condition worsened while the other received attention. Research demonstrates that relapse rates drop dramatically when both conditions receive simultaneous treatment rather than sequential or separate care. The feedback loop continues because each untreated condition sabotages progress in the other, making it mathematically impossible for single-focused treatment to succeed.
Psychiatric Symptoms That Masquerade as Addiction Problems
Clinicians without dual diagnosis training frequently misinterpret psychiatric symptoms as character flaws or insufficient motivation in recovery. Insomnia that stems from bipolar disorder receives treatment as poor sleep hygiene rather than a medication adjustment. Irritability caused by untreated anxiety gets labeled as resistance to treatment. Someone with ADHD struggles to follow treatment plans not because they lack commitment but because executive function deficits make sequential steps feel overwhelming. A person with schizophrenia stops taking antipsychotic medication and increases substance use, but the program attributes this to addiction rather than recognizing that untreated psychosis drives self-medication. These misdiagnoses delay proper treatment by months or years. The solution requires screening for both conditions simultaneously and adjusting interventions when progress stalls. If someone’s cravings spike despite consistent therapy, the assessment must include whether depression worsened, anxiety increased, or sleep deteriorated rather than assuming relapse is imminent. Housing instability, which affects 10 to 20 percent of people with dual disorders according to national estimates, compounds these challenges because unstable housing triggers psychiatric symptoms while making medication adherence nearly impossible. Practical recovery means addressing the psychiatric symptom directly through medication adjustment, increased therapy frequency, or psychiatric hospitalization if needed, rather than intensifying addiction-focused interventions that cannot touch the underlying mental health problem.
Extended Treatment Timelines That Support Real Change
Sustainable recovery for dual diagnosis requires treatment timelines measured in years, not months, and coping strategies that address both conditions in integrated ways. Standard 28-day or 90-day programs do not provide sufficient time to stabilize psychiatric medications, establish therapy relationships, and build genuine behavioral change. Integrated treatment delivers small overlapping changes over extended periods, which means someone might stabilize mood in month two while simultaneously building coping skills for cravings in month three. Cognitive behavioral therapy adapted for dual diagnosis teaches people to recognize how psychiatric symptoms trigger substance use and how substance use worsens psychiatric symptoms, breaking the cycle at both points. Employment and housing support matter intensely because instability in these areas directly undermines mental health and recovery; people with dual diagnosis show dramatically better outcomes when treatment includes supported employment services and housing assistance. Medication management requires ongoing adjustment because brain chemistry changes as someone stops using substances, meaning doses that worked in month one may need modification in month three. Long-term contact with treatment providers prevents the dangerous period after discharge when people lose support and symptoms resurface. Practical coping strategies include specific sleep protocols for people with bipolar disorder, structured daily routines for those with ADHD, grounding techniques for trauma survivors, and carefully timed substance use counseling that does not begin until psychiatric stability exists.
Coping Strategies That Address Both Conditions
Recovery plans that work acknowledge that someone with depression and alcohol dependence cannot simply stop drinking and expect their brain chemistry to correct itself; they need medication, therapy, lifestyle structure, and ongoing support working in concert. Effective coping strategies target the intersection of mental health and addiction rather than treating each separately. Sleep protocols matter because insomnia fuels both depression and substance cravings; someone with bipolar disorder needs consistent sleep schedules and sometimes medication adjustments to prevent mood episodes that trigger relapse. Structured daily routines help people with ADHD maintain medication adherence and therapy attendance while reducing the chaos that drives substance use. Grounding techniques (such as the 5-4-3-2-1 sensory method) help trauma survivors manage flashbacks and anxiety without turning to substances. Substance use counseling that begins only after psychiatric stability exists prevents the common scenario where someone receives addiction lectures while experiencing untreated panic or depression, making the counseling feel irrelevant or impossible to apply. These integrated strategies work because they interrupt the feedback loop at multiple points simultaneously rather than addressing one condition while the other deteriorates.
Final Thoughts
Dual diagnosis and addiction treatment succeeds when both conditions receive simultaneous attention from clinicians trained to address the feedback loop between mental health and substance use. The statistics are clear: roughly 10 million American adults struggle with co-occurring disorders in any given year, yet most still encounter fragmented care systems that treat these conditions separately. This approach fails because untreated psychiatric symptoms drive relapse, and untreated substance use destabilizes mental health.
Integrated treatment changes this outcome by coordinating medication management, counseling, employment support, and housing assistance through a single treatment team working from one coherent plan. Research from SAMHSA and the Dartmouth Psychiatric Research Center demonstrates that this model reduces hospitalization, lowers relapse risk, and improves employment and housing stability compared to traditional single-focus programs. Our team at Addiction Resource Center understands that dual diagnosis and addiction require a completely different treatment approach than single-condition recovery.
If you struggle with dual diagnosis and addiction, reaching out for help is the first step toward breaking the feedback loop that keeps you trapped. Contact Addiction Resource Center today to begin integrated treatment that addresses your complete picture rather than treating isolated symptoms.