Treat co-occurring disorders with integrated mental health care for stronger recovery outcomes.
About 9.2 million American adults struggle with both addiction and mental health conditions simultaneously. Yet most treatment programs focus on one problem at a time, leaving the other to fester and sabotage recovery.
At Addiction Resource Center, we’ve seen firsthand how co-occurring disorder care transforms outcomes when mental health and addiction treatment happen together, not separately. This blog post shows you why integrated treatment works and how to find it.
Understanding Co-occurring Disorders and Their Prevalence
About 9.2 million American adults struggle with both addiction and mental health conditions simultaneously. Most treatment programs focus on one problem at a time, leaving the other to worsen and sabotage recovery.
What Exactly Are Co-occurring Disorders
Co-occurring disorders mean a person has both a substance use disorder and a mental health condition at the same time. This isn’t two separate problems that happen to exist in one person. Depression, anxiety, PTSD, bipolar disorder, and ADHD all appear together with addiction more often than they appear alone. The data backs this up: roughly 45% of adults with any mental disorder have two or more conditions, according to research from Kessler and colleagues. Among people with substance use disorders, about 20% also have a mental illness-three times higher than the general population rate of 6%.
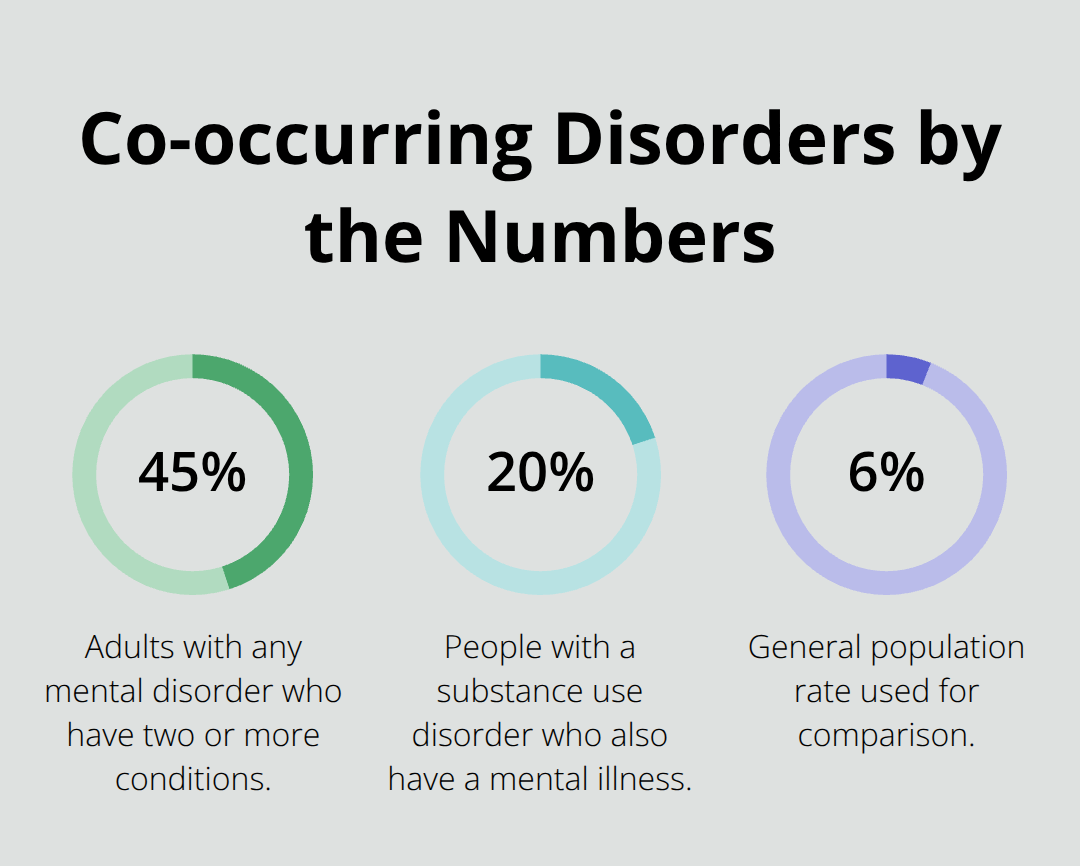
In clinical settings where people seek treatment, the numbers climb even higher. Around 36% to 40% of young adults with a serious mental health condition meet criteria for a substance use disorder as well.
Why Single-Disorder Treatment Fails
Treating addiction without addressing depression is like patching a roof while ignoring the foundation. A person stops drinking but the underlying depression remains untreated, so cravings intensify and relapse becomes almost inevitable. Research from multiple randomized controlled trials shows that integrated treatment produces significantly greater improvements in psychiatric symptoms, particularly PTSD, compared with treating each disorder separately. Yet many treatment programs still operate as if mental health and addiction are unrelated problems. This fragmented approach leaves clients bouncing between an addiction counselor and a mental health therapist who don’t communicate, don’t coordinate medication, and don’t adjust treatment based on progress in the other area. The result: higher relapse rates, increased emergency room visits, and more hospitalizations. Studies show that people with co-occurring disorders who receive integrated care have better psychiatric outcomes, though substance use improvements are comparable between integrated and non-integrated models. The real advantage lies in treating the psychiatric symptoms that drive continued use.
Depression and Anxiety Create Relapse Cycles
Depression appears in roughly 23.6% of overdose deaths, and the connection isn’t coincidental. When someone with both depression and alcohol use disorder stops drinking, the depression often worsens during early recovery because alcohol had been self-medicating the mood problem. Without antidepressant medication or therapy addressing the depression directly, the person experiences unbearable emotional pain and returns to drinking for relief. Anxiety works the same way. Generalized anxiety disorder affects about 2% of the population in any given year, but among people with substance use disorders, anxiety rates climb substantially higher (with lifetime anxiety prevalence reaching 38% in women and 27% in men). Anxiety and addiction feed each other: substance use temporarily quiets anxiety, but withdrawal and continued use intensify it, creating a vicious cycle. Treatment that addresses only the addiction leaves the anxiety untreated, and the person self-medicates again. This is why integrated treatment that combines medication management with behavioral therapy produces better long-term outcomes than either approach alone.
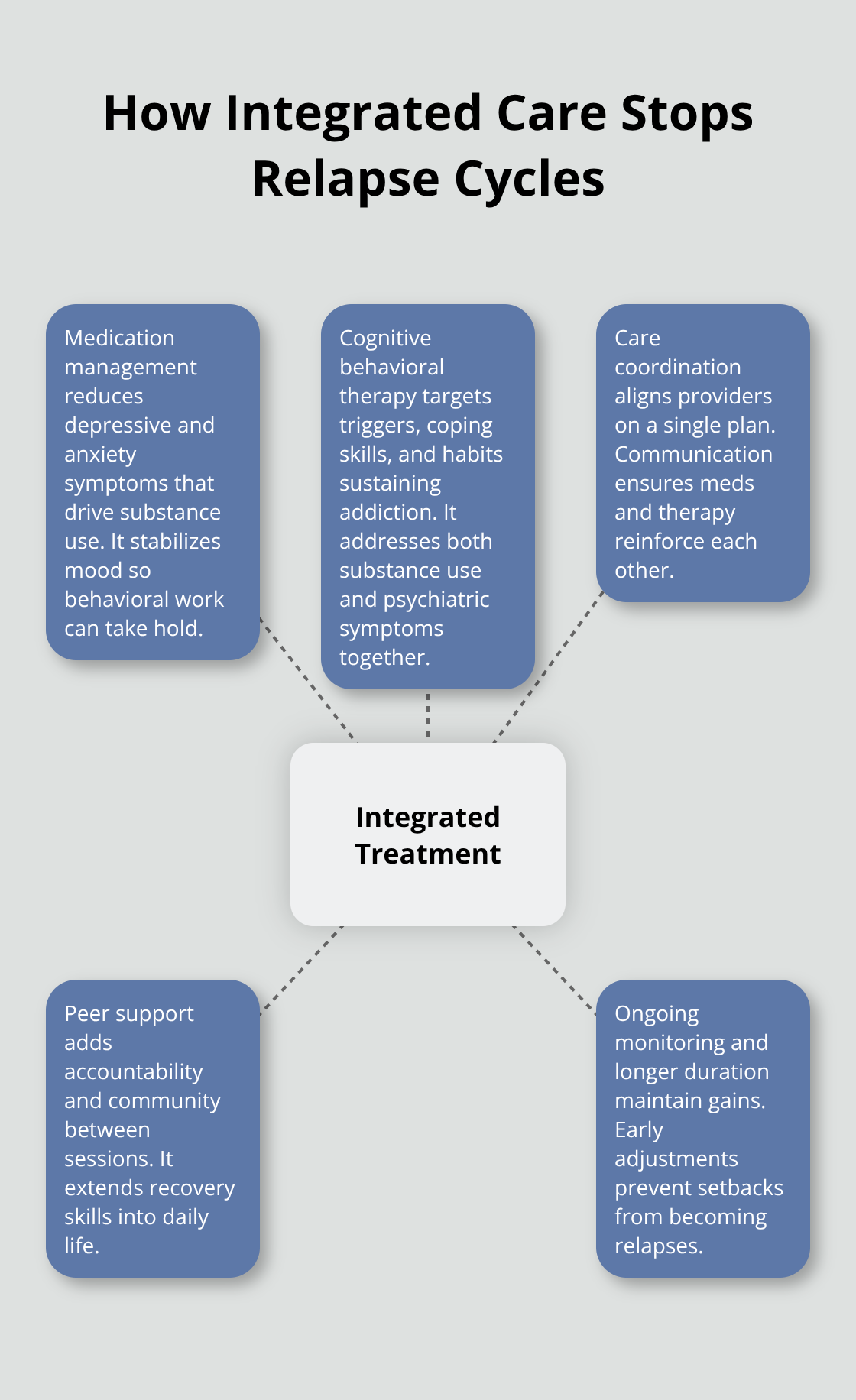
How Integrated Care Breaks the Cycle
When mental health treatment and addiction treatment happen simultaneously, outcomes shift dramatically. A person receives antidepressants or anti-anxiety medication while also working with a therapist on both the addiction and the underlying mental health condition. The medication reduces the psychiatric symptoms that drive substance use, while therapy addresses the behavioral patterns and coping skills that support recovery. This dual approach prevents the relapse cycles that single-disorder treatment allows to flourish. The person no longer faces the choice between untreated depression and untreated addiction-they address both at once. Research consistently shows that this integrated model reduces psychiatric symptoms more effectively than treating disorders separately, and it keeps people engaged in treatment longer.
The next section explores the specific treatment approaches that make this integration work.
The Impact of Untreated Mental Health on Addiction Recovery
How Depression Fuels Relapse
Untreated depression doesn’t just coexist with addiction-it actively drives relapse. When someone enters addiction treatment without addressing the underlying depression, they face an impossible situation: the psychiatric symptoms that triggered substance use in the first place remain untreated. Depression reduces motivation and increases hopelessness, making early recovery feel unbearable. Research shows that individuals with both depression and alcohol use disorder experience hazard ratios of 1.89 for drug-related overdoses compared to those with addiction alone. The mechanism is straightforward: a person stops drinking but without antidepressant medication or evidence-based therapy, the depression intensifies during early abstinence. Within weeks, emotional pain becomes so severe that returning to substance use feels like the only escape. Depression appears in roughly 23.6% of overdose deaths-a connection that reflects this relapse cycle.
Anxiety and Trauma Perpetuate the Cycle
Anxiety creates constant dread and physical tension that people historically managed through substance use. Generalized anxiety disorder affects approximately 2 percent of the population annually, but among people with substance use disorders, comorbidity rates spike dramatically (with lifetime anxiety prevalence reaching 38% in women and 27% in men). The person quits using, anxiety floods back without treatment, and they relapse to silence the unbearable internal noise. Trauma compounds this dynamic further. PTSD frequently accompanies substance use disorder, and trauma-focused therapy must happen alongside addiction treatment to address both the hyperarousal and the conditioned responses that trigger cravings. Without trauma work, a person remains trapped in survival mode, using substances to numb flashbacks and nightmares.
Why Integrated Treatment Produces Superior Outcomes
Integrated treatment that addresses mental health and addiction simultaneously produces measurably different results. Research from multiple randomized controlled trials demonstrates that people receiving integrated care experience significantly greater reductions in psychiatric symptoms, particularly PTSD symptoms, compared to those in traditional single-disorder programs. Personalized treatment planning that includes addressing co-occurring mental health conditions significantly improves long-term recovery outcomes. Medication management combined with trauma-informed cognitive behavioral therapy creates a synergistic effect that neither approach achieves alone. When an antidepressant reduces depressive symptoms while a therapist teaches coping skills for both addiction triggers and anxiety symptoms, the person gains real traction in recovery.
The Role of Treatment Duration and Coordination
Treatment duration matters significantly-longer engagement in integrated outpatient care with sustained monitoring reduces relapse and psychiatric hospitalization more effectively than short-term programs. The strongest outcomes occur when treatment combines pharmacotherapy with behavioral interventions like motivational interviewing and contingency management, adjusted specifically for the person’s constellation of symptoms. Fragmented care-where an addiction counselor and psychiatrist work independently without communication-produces worse outcomes. The person receives conflicting advice, medication changes that lack coordination with behavioral work, and no unified treatment plan that addresses how each condition affects the other. This coordination gap explains why many people cycle through multiple treatment attempts before finding an approach that actually works.
Moving Toward Integrated Solutions
The evidence is clear: mental health conditions and addiction cannot be treated as separate problems. The next section explores the specific integrated treatment approaches that break these relapse cycles and produce lasting recovery.
Integrated Treatment Approaches for Co-occurring Disorders
Medication as the Foundation of Dual Diagnosis Care
Medication combined with therapy forms the foundation of effective co-occurring disorder care, and the evidence overwhelmingly supports this pairing. When someone has both depression and alcohol use disorder, an SSRI antidepressant like sertraline combined with cognitive behavioral therapy produces significantly greater reductions in both drinking and depressive symptoms than either treatment alone. The medication addresses the neurochemistry driving the depression, while therapy teaches the person to recognize triggers, manage cravings, and build new coping patterns. This isn’t theoretical-it’s the standard approach at programs treating serious dual diagnoses.
Extended-release formulations matter significantly. For people with ADHD and substance use disorder, extended-release stimulant medications carry substantially lower diversion risk than immediate-release forms, making them the safer choice when carefully monitored. Clinicians track prescription pickup patterns, conduct regular urine screens, and watch for signs of misuse. Some providers avoid stimulants entirely, but modest-dosed, supervised stimulant therapy actually reduces substance use in ADHD patients with addiction compared to leaving ADHD untreated.
Anti-anxiety medications require a different approach. Benzodiazepines carry high abuse potential and clinicians generally discourage them, but buspiron can reduce both anxiety and alcohol consumption without the addiction risk. For anxiety paired with opioid dependence, cognitive behavioral therapy combined with pharmacotherapy improves abstinence days more effectively than either approach alone. The medication piece isn’t optional-it’s what allows the behavioral work to actually stick.
Cognitive Behavioral Therapy for Dual Diagnosis
Cognitive behavioral therapy for dual diagnosis works differently than standard addiction counseling because it addresses both the addiction patterns and the underlying mental health symptoms simultaneously. A therapist doesn’t just teach relapse prevention for substance use; they also help the person identify how depression or anxiety triggers cravings, develop coping skills for both conditions, and recognize the connection between emotional states and substance use.
This integrated approach produces measurable results. Research shows that CBT combined with antidepressants yields significant improvements in depression, anxiety, substance use, and coping skills. The therapist adjusts treatment based on how each condition affects the other, rather than treating them as separate problems that happen to exist in one person. This coordination prevents the relapse cycles that single-disorder treatment allows to flourish.
Peer Support and Community-Based Programs
Peer support and community-based programs serve a different function than clinical treatment but remain essential to long-term recovery. Dual Recovery Anonymous and other co-occurring-focused mutual-help groups provide ongoing accountability and community after formal treatment ends. Alcoholics Anonymous has approximately 61,000 meetings and 1.3 million members in the United States, offering accessible recovery support, though traditional AA doesn’t specifically address mental health medication or psychiatric symptoms.
The strongest outcomes occur when someone receives medication management and therapy from a coordinated clinical team while also participating in peer support. This combination addresses the biological, psychological, and social dimensions of recovery. Someone with co-occurring depression and addiction typically needs at least several months of consistent treatment, not weeks. Longer engagement in integrated outpatient care with sustained monitoring reduces relapse and psychiatric hospitalization more effectively than short-term programs.
Why Coordination Between Providers Matters
Treatment coordination separates effective dual diagnosis care from fragmented approaches that fail. When an addiction counselor and psychiatrist work independently without communication, the person receives conflicting advice, medication changes that lack coordination with behavioral work, and no unified treatment plan that addresses how each condition affects the other. This coordination gap explains why many people cycle through multiple treatment attempts before finding an approach that actually works.
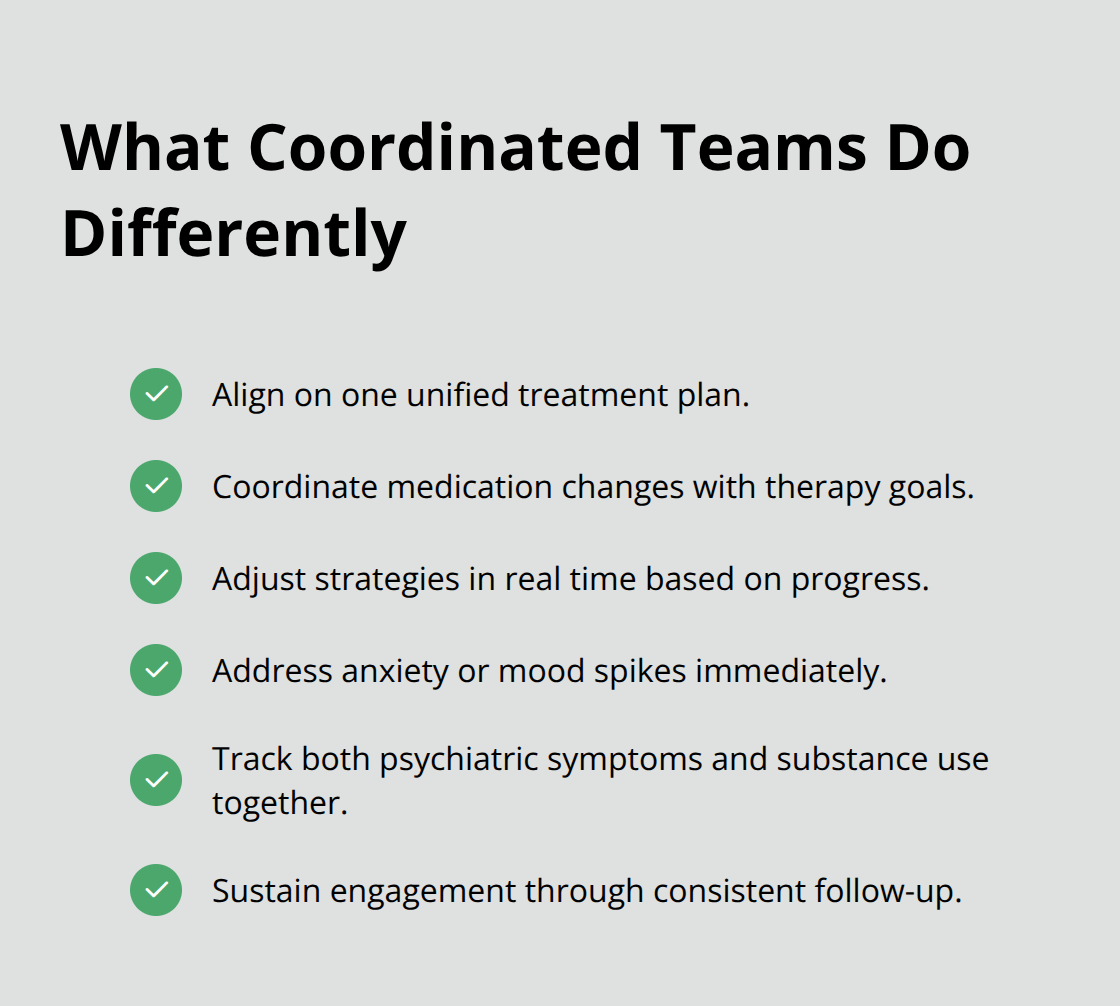
Coordinated teams adjust treatment based on progress in both areas simultaneously. If someone shows improvement in depression but continued substance use, the team modifies the approach rather than assuming the person lacks motivation. If anxiety spikes during early recovery, the team addresses it immediately rather than waiting for the next appointment. This responsiveness keeps people engaged and prevents the hopelessness that derails recovery.
Final Thoughts
The evidence is unambiguous: integrated co-occurring disorder care produces measurably better outcomes than treating addiction and mental health separately. People who receive coordinated medication management, behavioral therapy, and peer support experience greater reductions in psychiatric symptoms, longer engagement in treatment, and lower relapse rates. This isn’t a marginal improvement-it’s the difference between cycling through failed treatment attempts and achieving sustained recovery.
Your mental health condition and your addiction feed each other relentlessly, so treating one while ignoring the other guarantees failure. Depression intensifies cravings, anxiety drives substance use, and trauma creates hypervigilance that only substances seem to quiet. Integrated treatment breaks this cycle by addressing both conditions simultaneously through medication, therapy, and community support working in coordination. Look for programs that employ coordinated teams, offer medication management alongside therapy, and provide ongoing monitoring rather than short-term interventions.
We at Addiction Resource Center understand that recovery requires treating the whole person, not just the addiction. Contact our team today to learn how our integrated approach to substance abuse treatment and mental health support can help you achieve lasting recovery.