You may be staring at a phone that never leaves your hand. You're checking for signs your loved one is safe, replaying the last conversation, wondering whether today is the day things get worse. Families often reach this point after months or years of pleading, covering, arguing, and hoping that one honest talk will finally …
You may be staring at a phone that never leaves your hand. You're checking for signs your loved one is safe, replaying the last conversation, wondering whether today is the day things get worse. Families often reach this point after months or years of pleading, covering, arguing, and hoping that one honest talk will finally break through.
What makes this moment so painful is that love alone hasn't been enough to change the pattern. You may know your loved one is suffering, and they may know it too, but addiction can still keep everyone stuck in confusion, fear, and avoidance. Staging an intervention can help, but only when it's approached with care, structure, and emotional discipline.
Table of Contents
- An Intervention Is an Act of Love Not War
- Determining Readiness and Assembling Your Team
- Crafting a Detailed and Compassionate Plan
- Navigating the Meeting and Handling Resistance
- From Yes to Recovery Immediate Treatment and Aftercare
- Frequently Asked Questions About Interventions
An Intervention Is an Act of Love Not War
Most families don't begin with an intervention. They begin with private talks in the kitchen, promises after crises, money lent with conditions, and late-night drives to pick someone up when things fall apart again. By the time people consider staging an intervention, they're often exhausted and carrying a mix of grief, anger, guilt, and dread.
That emotional mix matters. If the family walks into the room hoping to force a confession, punish the person, or unload months of resentment, the meeting usually becomes a fight about tone instead of a path toward treatment. A useful intervention is different. It says, clearly and together, “We love you, we see the harm, and we are prepared to help right now.”
Media often portrays interventions as dramatic ambushes. Real ones work better when they are quiet, prepared, and rooted in dignity. The point isn't to corner someone. The point is to interrupt denial with a coordinated message from people whose concern can't be dismissed as random criticism.
An intervention works best when the family sounds united, calm, and serious, not shocked by its own feelings.
Families also need to understand that addiction rarely exists in isolation. Trauma, anxiety, depression, fear, and chronic stress often shape how a person uses substances and how the household responds. That's one reason broader family education matters. If your loved one also struggles with trauma-related symptoms, these tips for helping someone with PTSD can help you communicate with more steadiness and less reactivity.
The heart of staging an intervention is simple. Love needs structure. Without structure, families drift into pleading, bargaining, or shouting. With structure, they create a moment where concern is clear, help is ready, and the next step is no longer vague.
Determining Readiness and Assembling Your Team
An intervention should happen because the family is ready to act, not because everyone is panicking after the latest incident. Timing matters, but emotional readiness matters just as much. If the group isn't willing to stay aligned before, during, and after the meeting, it's too early.
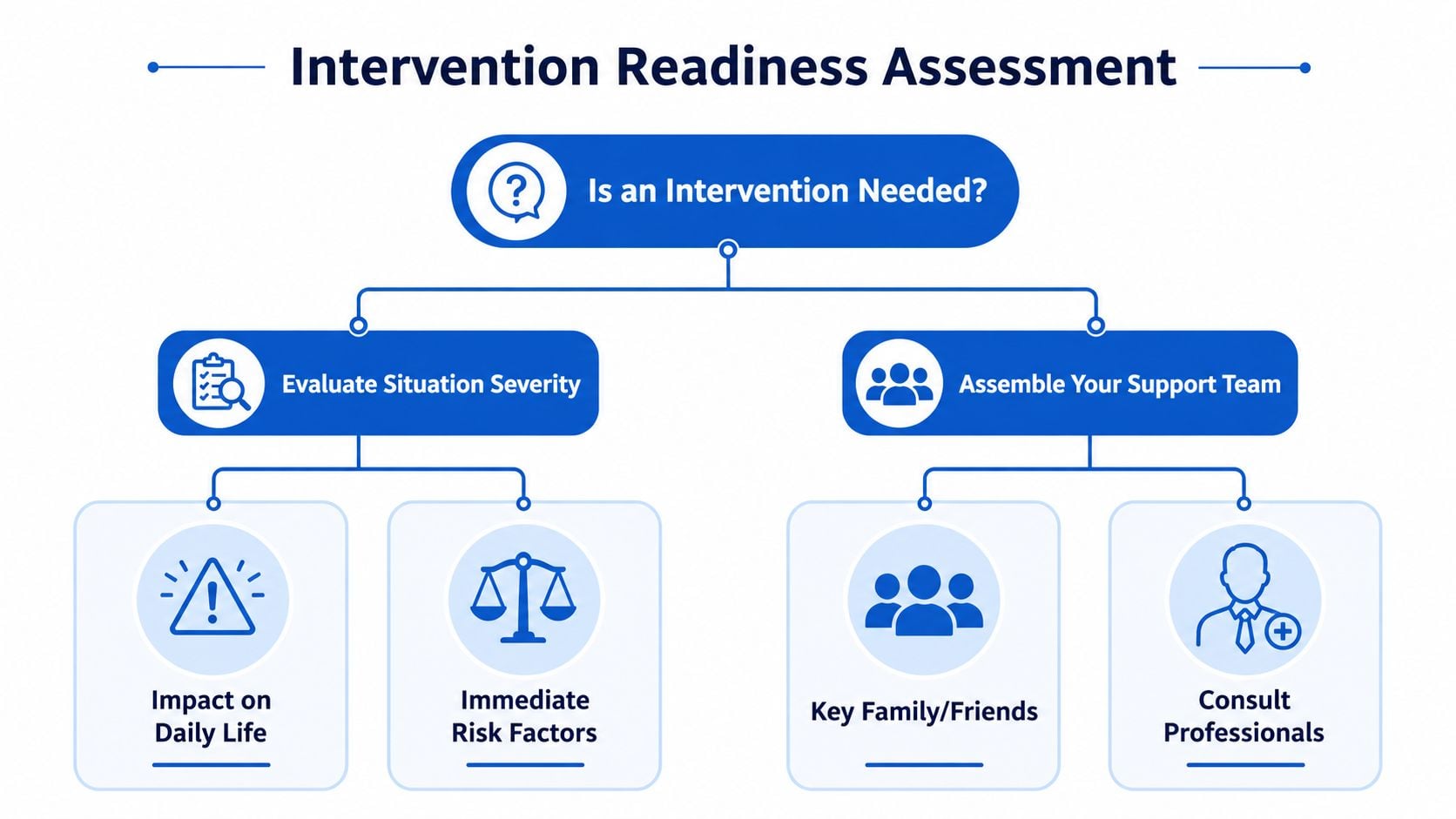
Read the situation before you call the meeting
Start with two questions. Is the substance use disrupting health, safety, work, parenting, or basic functioning? And can the family speak with one voice, even if the loved one becomes defensive?
Some signs point toward the need for a formal intervention:
- Repeated broken promises: They keep saying they'll cut back, stop, or get help, and the cycle continues.
- Escalating consequences: Daily life is becoming unstable, unsafe, or chaotic.
- Family paralysis: Everyone is worried, but no one knows what to do besides react to the latest crisis.
- Private conversations go nowhere: One-on-one talks end in denial, avoidance, or temporary peace without real change.
Emotional readiness means something equally practical. Participants must be willing to stop rescuing, stop improvising, and follow through on agreed boundaries if treatment is refused.
Choose a team that can stay steady
The ideal intervention team is small and credible. A structured, professionally guided intervention achieves an 80 to 90% success rate in convincing the individual to accept treatment, compared with 30% for unstructured approaches, and key methodology includes forming a 4 to 6 person team of significant individuals and rehearsing each participant's impact statement at least once, according to American Addiction Centers' intervention guide.
That number doesn't mean “the more people, the better.” It means discipline matters. A smaller group is easier to prepare, easier to manage, and harder for the loved one to split against itself.
Include people who are:
- Closely connected: Adult relatives, close friends, or others whose words carry emotional weight.
- Emotionally stable: They can stay composed even if the loved one lies, cries, or lashes out.
- Willing to rehearse: They'll prepare statements, listen to coaching, and avoid freelancing.
- Ready to follow through: They won't undermine the plan later by softening consequences.
Leave out people who are likely to escalate the room. That includes anyone who is intoxicated, volatile, resentful, or still actively enabling. It can also include people who mean well but can't stay on topic.
For some families, the harder preparation happens outside the intervention meeting itself. If codependent patterns have shaped the household for a long time, support around boundaries can change how the whole process unfolds. This overview of holistic therapy for codependency is useful for families who keep confusing care with overfunctioning.
Why professional guidance matters
A professional interventionist does more than “run the meeting.” They prepare the family for the emotional reality of the meeting. They help identify who should attend, who should sit out, what language is likely to provoke resistance, and where the plan is still too vague to work.
Practical rule: If the family cannot agree on one immediate treatment goal and one set of boundaries, don't schedule the intervention yet.
A trained mental health professional also protects the tone of the room. Families under stress often slide into lecturing or arguing. A good interventionist keeps the focus where it belongs: observed behavior, personal impact, clear treatment options, and consequences the family can realistically maintain.
Crafting a Detailed and Compassionate Plan
The intervention usually succeeds or fails before anyone enters the room. Planning is where families turn raw concern into something organized and usable. Without that work, people talk too long, speak from panic, or offer treatment as a loose future idea instead of a present choice.
Professional interventionists report that interventions succeed in 80% to 90% of cases when success is defined as the target individual accepting immediate help, and they attribute that result to rigorous planning, a dedicated team, rehearsed personal impact statements, and a specific, enforceable goal such as immediate admission to a treatment facility, according to the Association of Intervention Specialists.
Set the conditions for a safe conversation
The meeting should happen when the person is sober, medically stable, and most likely to be able to listen. Choose a setting that feels calm and familiar, not theatrical or threatening. The location should support privacy and focus, but it should not feel like a trap.
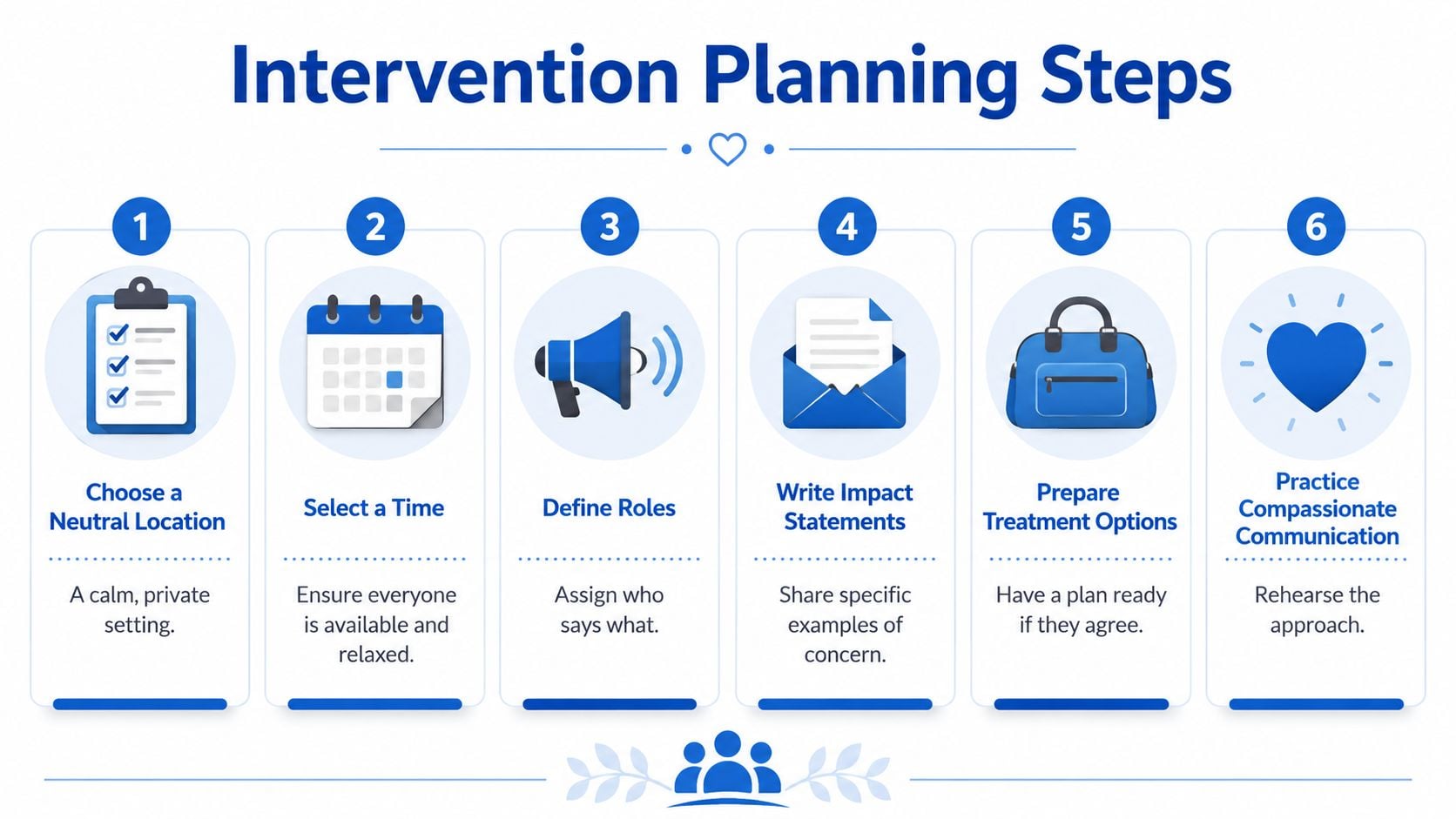
A strong plan covers these practical details:
| Planning area | What good planning looks like |
|---|---|
| Timing | The loved one is sober and the team can be fully present |
| Location | Calm, neutral, private, and not chaotic |
| Roles | Everyone knows who opens, who reads when, and who closes |
| Goal | One clear ask tied to immediate treatment |
| Logistics | Transportation, admission contact, and essentials are ready |
Rehearsal matters for tone as much as content. People need to hear how they sound when they're anxious. A sentence that feels heartfelt in your head can land as blame when spoken out loud.
Write statements that are honest and usable
Each person should prepare a short statement based on direct observation and personal impact. Families often slip into accusation at this point. The language needs to stay grounded.
Use “I” statements. Name what you've seen. Name how it affected you. State what you hope happens next.
Here's the difference:
- Less helpful: “You're selfish and you ruin every family event.”
- More helpful: “I felt scared and ashamed when you drove after drinking. I've been carrying that fear ever since.”
- Less helpful: “You never care about anyone.”
- More helpful: “I miss who you are when you're well, and I'm not willing to keep pretending this isn't hurting all of us.”
A strong impact statement usually includes:
- A specific incident you personally witnessed.
- Your emotional response to that incident.
- A boundary you will keep if treatment is refused.
- A statement of love that keeps the message human.
Speak to the person you love, not to the behavior you hate.
Keep the statements short. Long speeches invite rebuttal. Clear statements create a record of shared reality.
Make the treatment path immediate and concrete
Families often do strong emotional preparation and then weaken at the most important point. They ask their loved one to “get help” without defining where, when, or how. That leaves room for delay, bargaining, and escape.
The treatment option must be arranged in advance. That means confirming the program, understanding admission steps, knowing who to call, and preparing transportation so “yes” can become movement, not another discussion.
Your planning checklist should include:
- A specific level of care: Detox, residential treatment, outpatient support, or another clinically appropriate option.
- Immediate contact information: One point person for admission and one backup.
- Travel readiness: Who drives, who rides along, and what route keeps things simple.
- Basic packing plan: Identification, medications, approved clothing, and essentials.
- Family boundaries: What changes today if the person says no.
Consequences should be proportional and real. They are not threats. They are changes the family will make to stop protecting the addiction. That could mean ending financial support, refusing to provide housing under unsafe conditions, or no longer covering up legal, work, or relationship consequences.
The rule is simple. Never name a consequence you won't keep. Empty consequences don't create influence. They teach the loved one that the family will collapse under pressure.
Navigating the Meeting and Handling Resistance
The meeting itself is usually emotionally intense, but it should not feel chaotic. Calm is contagious when the team has prepared well. So is panic when the team hasn't.

How to hold the room
Begin clearly. Tell your loved one that everyone is there because they care and because the situation can't continue as it has been. Then move into the prepared order. One person speaks at a time. No interruptions. No side arguments.
The group's job is to lower chaos without lowering clarity. That means sitting with tears, anger, silence, and denial without getting pulled into debate. If your loved one starts challenging details, arguing history, or redirecting blame, the team should return to the prepared statements and the immediate treatment offer.
Helpful responses sound like this:
- “I hear that you disagree. I still need to say what I've experienced.”
- “We're not here to argue every event. We're here because we want you to accept help today.”
- “You don't have to agree with all of us. You do need to hear that we're aligned.”
What resistance usually sounds like
Resistance often comes in recognizable forms. Denial. Bargaining. Anger. Blame-shifting. Promises to do something later. Emotional collapse designed, consciously or not, to stop the meeting.
A compassionate approach matters. Common pitfalls include staging an intervention when the person is under the influence, including unstable or highly emotional participants, and omitting a pre-researched treatment plan. The same source notes that about 65% success is seen with the CRAFT model, which is superior to standard intervention's about 30% when unstructured, according to River Rock Treatment's guidance on intervention dos and don'ts.
CRAFT matters because it shifts the family away from attack. Instead of trying to win through force, shame, or superior logic, the family uses consistent responses, emotional connection, and healthier reinforcement. In practice, that means you don't try to out-argue addiction in the room. You stay warm, direct, and repetitive.
“We love you. We're prepared to help today. We won't keep participating in what's harming you.”
If the person becomes threatening or the situation feels unsafe, stop the meeting. Safety comes first. An intervention is never a test of endurance.
Stay united if they refuse help
A refusal hurts, especially after so much preparation. But the intervention still has value if the family follows through. In many cases, the first meeting breaks denial open even if the answer isn't immediate acceptance.
If your loved one says no:
- Keep responses brief: Don't chase them with new arguments.
- Restate the offer once: The treatment option remains available now.
- Implement boundaries: Each person follows the plan already agreed upon.
- Avoid rescue afterward: Don't erase the impact of refusal by returning to old patterns that same day.
The meeting is only one moment. The family's consistency afterward often determines whether that moment leads anywhere.
From Yes to Recovery Immediate Treatment and Aftercare
A yes is important, but it's fragile. Once your loved one agrees to treatment, move. Don't turn the next hour into a family debrief, an extended goodbye, or a chance to sleep on the decision.
Move quickly after yes
The family should already know who is making the call, who is handling transportation, and what basic belongings are needed. The person should move directly into the next clinical step without unnecessary delays. Waiting gives fear time to return.
During intake, treatment providers typically gather history, assess substance use and mental health needs, review medications, and determine the safest level of care. For some people that begins with detox. For others, it may involve residential care, medication-assisted treatment, or outpatient support. The important point is continuity. Momentum protects commitment.
A practical same-day checklist helps:
- Admission contact ready: One person handles communication with the facility.
- Transportation arranged: No debate in the driveway.
- Essentials packed: Keep it simple and treatment-appropriate.
- Family contact expectations clarified: Know what communication may look like in the first phase of care.
Recovery support has to include the family
Families often exhale once treatment begins, then discover how much healing still needs to happen at home. The intervention may have been aimed at one person, but the recovery process touches the entire system around them.
That's why aftercare planning matters for both sides. The loved one needs relapse prevention, structure, and continuing support. The family needs education, boundaries, and often its own therapy to stop revolving around crisis. In homes where language or cultural context affects access to care, it may help to find multilingual addiction therapy so communication doesn't become another barrier to treatment engagement.
Recovery gets stronger when the family stops managing chaos and starts supporting treatment.
Early recovery can be emotionally uneven. Some days bring relief. Others bring resentment, fear, or old family roles rushing back in. That doesn't mean treatment isn't working. It means the family needs a plan that lasts longer than the intervention itself.
Frequently Asked Questions About Interventions
What if they walk out
If your loved one leaves, the meeting isn't automatically a failure. The key question is what the family does next. Don't chase, bargain, or soften everything that was said in order to reduce your own discomfort.
Send one clear message if needed: help is available, and the boundaries still stand. Then hold the line. Consistency is what gives the intervention meaning after the meeting ends.
Is an intervention a legal process
Usually, no. An intervention is a private family effort to encourage treatment. It isn't a court hearing, and it doesn't create legal authority over an adult because the family is worried.
Legal questions can arise in specific situations, such as guardianship, acute safety crises, or mandated care. Those situations need direct professional guidance. Families shouldn't assume an intervention itself gives them power to compel treatment.
Is hiring an interventionist worth it
In many families, yes. Not because the professional says anything magical, but because they give the process containment. They coach the team, improve the language, challenge weak boundaries, and reduce the chance that the meeting turns into a circular argument.
They also help with trade-offs. For example, some loved ones need a direct, same-day intervention. Others respond better when the family has already begun changing enabling patterns before the formal meeting occurs. A professional can tell the difference more clearly than a frightened family usually can.
Staging an intervention is one of the hardest things a family may ever do. It asks people to stay loving without becoming passive, and to stay firm without becoming cruel. That balance is what makes the process compassionate, and what gives it the best chance to open the door to treatment.
If your family is at the point where waiting feels dangerous, Addiction Resource Center LLC offers compassionate drug and alcohol treatment in Yuba City with medically supervised detox, MAT, residential rehab through Ona Treatment Center, IOP in person and via telehealth, and individualized aftercare planning. Their team includes medical, counseling, and recovery professionals, and they welcome adults, families, insured patients, and Tricare beneficiaries who need a clear next step now.