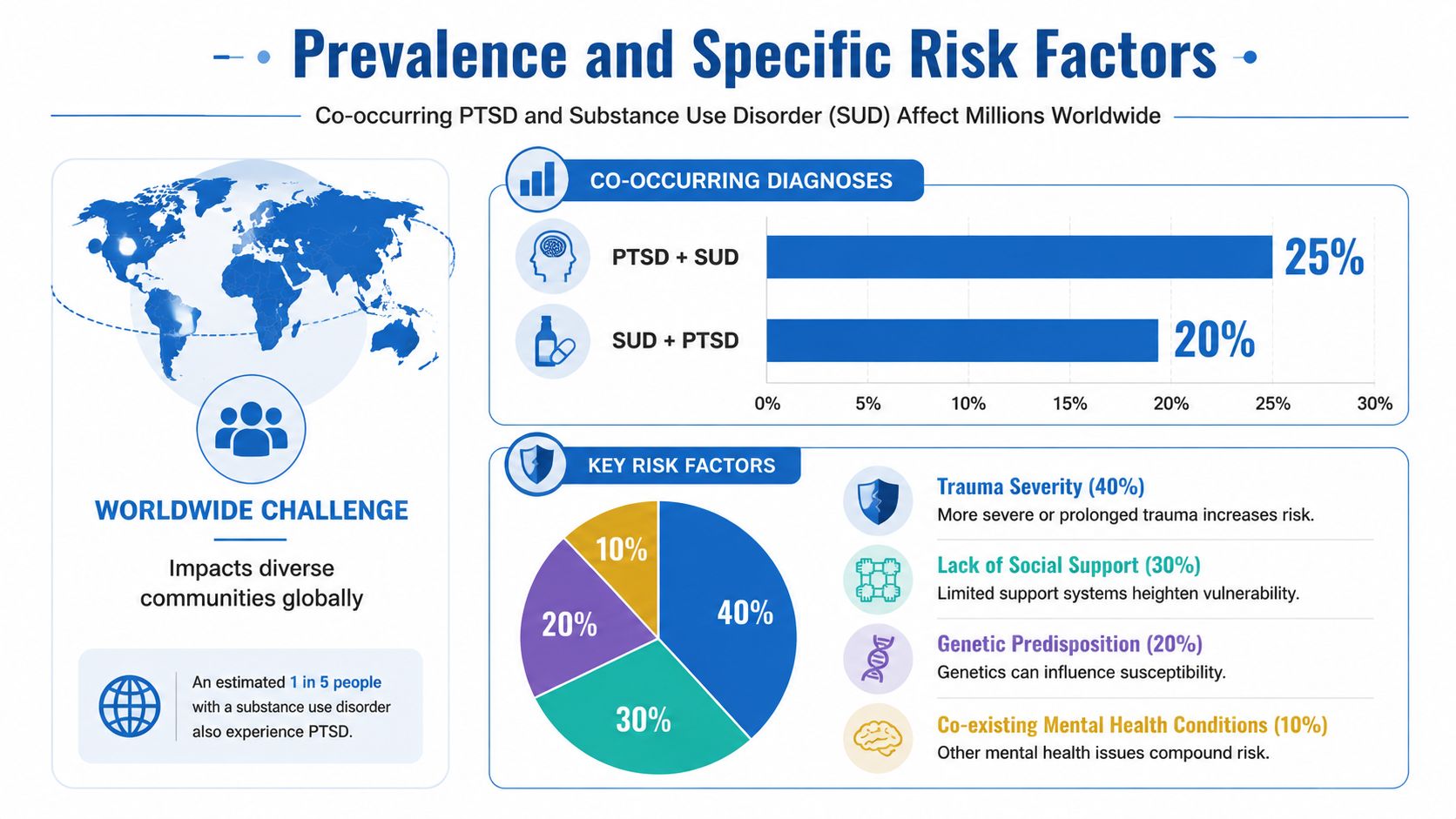
Over 4 out of 10 adults with PTSD also have problems with drug or alcohol use, and among adults with a substance use disorder, 12% to 34% have PTSD according to the International Society for Traumatic Stress Studies fact sheet. That changes the conversation right away. PTSD and substance use aren't separate problems that just …

Over 4 out of 10 adults with PTSD also have problems with drug or alcohol use, and among adults with a substance use disorder, 12% to 34% have PTSD according to the International Society for Traumatic Stress Studies fact sheet. That changes the conversation right away. PTSD and substance use aren't separate problems that just happen to show up together sometimes. For many people, they are tightly connected.
If this is affecting you or someone you love, it can feel confusing. Families often ask, “Did the trauma cause the addiction?” People struggling themselves often ask, “Why can't I just stop using if I know it's making things worse?” Both are fair questions.
PTSD is what can happen after overwhelming trauma. A person may have nightmares, flashbacks, panic, irritability, emotional numbness, trouble sleeping, or a constant sense that danger is close. Substance Use Disorder means alcohol or drugs have started to take control, despite harm to health, work, relationships, or safety. When both happen together, clinicians call it a co-occurring disorder or dual diagnosis.
The most useful starting point is this: many people use substances because they work, at least briefly. They numb fear, quiet intrusive memories, slow down a racing mind, or help someone sleep for a few hours. The problem is that the relief doesn't last, and the cycle gets stronger.
Table of Contents
- Understanding the Link Between Trauma and Addiction
- The Vicious Cycle of PTSD and Substance Use
- Prevalence and Specific Risk Factors
- Why Co-Occurring Disorders Complicate Recovery
- Evidence-Based Treatments That Heal Both Conditions
- How Addiction Resource Center Provides Integrated Care
- Your Next Steps to Begin Healing in Yuba City
Understanding the Link Between Trauma and Addiction
Nearly half of people with PTSD also struggle with alcohol or drug use, as noted earlier in this article. That overlap is common enough that clinicians expect to see the two conditions together.
This context is important because people often get blamed for reactions that make sense once trauma is part of the picture. A person who drinks after nightmares, uses pills to quiet panic, or smokes marijuana to calm a constantly activated nervous system may be trying to get through the day with the tools available to them. The behavior can still be dangerous. It is also understandable.
What co-occurring disorders really mean
Co-occurring disorders are closely connected problems, not two separate labels sitting in the same chart. PTSD can raise fear, tension, insomnia, and emotional pain. Substance use can add withdrawal, shame, conflict, memory problems, and unstable sleep. The result is a feedback loop where each condition gives the other more fuel.
A helpful way to understand it is to picture a smoke alarm that has become too sensitive. PTSD can make the brain and body react to reminders of danger as if the threat is happening right now. Alcohol or drugs may seem like a quick way to turn down the volume. For a short time, that can feel like relief. Over time, it often makes the whole system less stable and harder to calm naturally.
Practical rule: If trauma symptoms and substance use feed each other, treatment needs to address both together.
Families often get caught in the wrong question. They ask whether the drinking should be treated first or the PTSD should be treated first. In daily life, those problems are usually tangled together. A flashback may lead to drinking. A night of drinking may worsen sleep, increase irritability, and make therapy harder the next day.
What people usually get wrong
A common misunderstanding is that substance use after trauma is mainly about pleasure, recklessness, or weak willpower. For many trauma survivors, it works more like emotional anesthesia. The goal is not to get high for fun. The goal is to feel less scared, less numb, less ashamed, or less overwhelmed.
That is the "why" behind the overlap, and it points toward the right kind of help. If the substance has been serving a purpose, even an unhealthy one, recovery has to offer safer ways to sleep, regulate emotions, and handle triggers. Generic advice to "just stop" usually misses the problem.
Integrated treatment is the practical next step. At Addiction Resource Center, that means looking at trauma symptoms and substance use in the same care plan so the person is not asked to solve one while the other keeps pulling them back.
The Vicious Cycle of PTSD and Substance Use
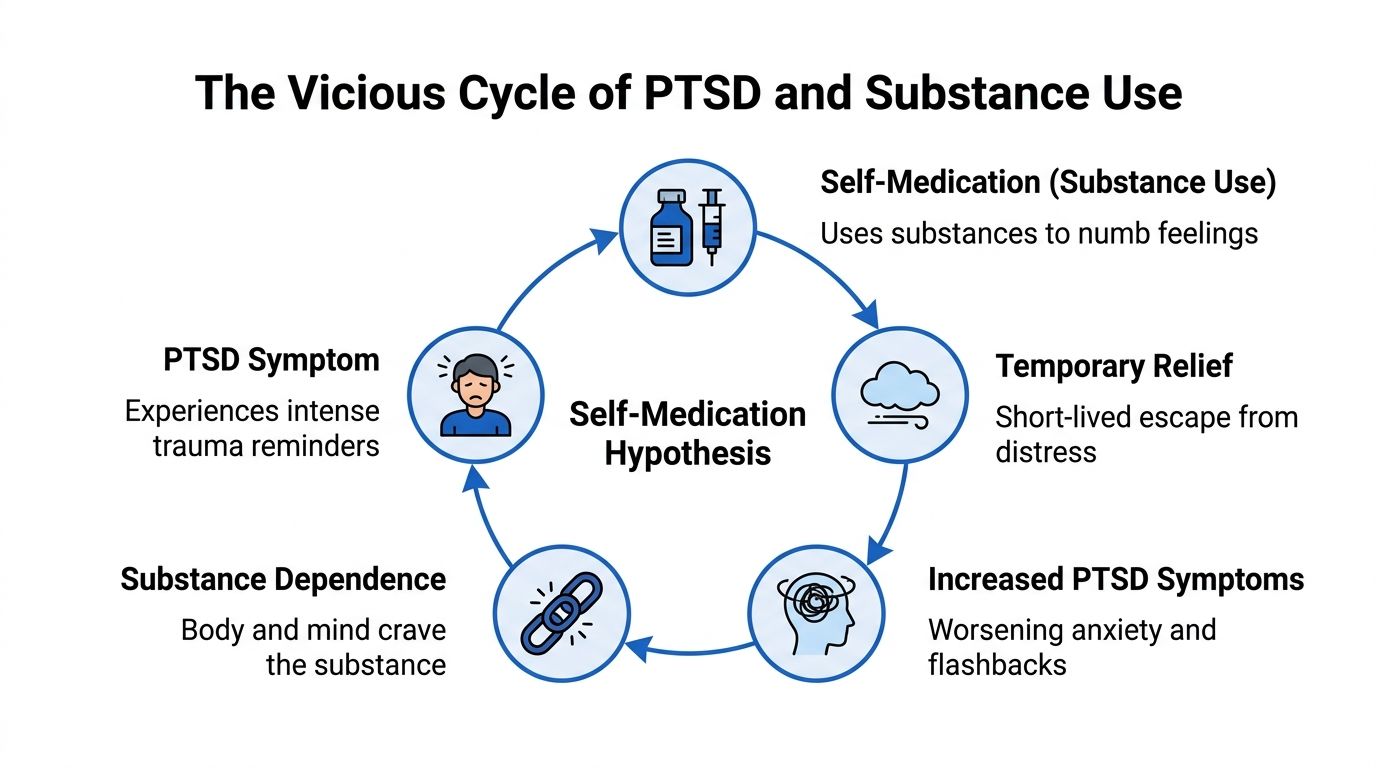
A lot of people know that trauma and addiction are connected, but they still don't understand how the cycle works day to day. The missing piece is usually self-medication.
Why substances can feel like relief
Start with a PTSD symptom. Someone hears a sound that reminds them of a traumatic event. Their chest tightens. Their thoughts race. They feel a flash of fear, shame, anger, or helplessness. They want that feeling to stop immediately.
A substance can provide a fast shift. Alcohol may dull intensity. Opioids may create distance from pain. Stimulants may temporarily override numbness or exhaustion. Marijuana may seem to soften hyperarousal for some people. In the moment, the brain learns something important: “This works.”
That lesson is powerful. The next time distress rises, the urge to use can show up faster and stronger.
Later in the cycle, many people notice these patterns:
- Triggers become linked to cravings. Trauma reminders don't just bring fear. They can also cue the urge to drink or use.
- Relief gets shorter. What worked early on often stops working as well.
- Consequences pile up. Missed work, relationship strain, hiding behavior, and shame create more stress.
- PTSD symptoms worsen. Sleep gets more disrupted, emotions get less predictable, and recovery feels farther away.
The result isn't weakness. It's conditioning.
A short video can help make this easier to picture in real life.
What changes in the brain and body
This cycle isn't only psychological. It also involves the body's stress systems. According to a review in Molecular Psychiatry, people with both conditions often show greater neuroendocrine dysregulation involving the hypothalamic-pituitary-adrenal, or HPA, axis, creating a stronger coupling between stress response and substance use than in people with only one disorder.
In plain language, the alarm system gets easier to trigger, and the brain learns to pair that alarm with substance use as a response. Over time, that can make stopping feel harder than outsiders expect.
When a person says, “I use because it's the only thing that calms me down,” that isn't a full solution, but it often is an honest description of the cycle they're trapped in.
A useful way to think about it is this:
| Part of the cycle | What the person experiences |
|---|---|
| Trauma reminder | Fear, numbness, panic, anger, shame |
| Substance use | Immediate drop in distress or shift in mood |
| After-effect | Cravings, guilt, conflict, rebound anxiety |
| Reinforcement | Stronger urge to repeat the same pattern |
Once families see the loop clearly, “just stop” starts to sound as unrealistic as telling someone with a panic attack to “just relax.”
Prevalence and Specific Risk Factors
PTSD and substance use do not cluster in certain groups by accident. The pattern usually reflects three forces working together: the type of trauma, how often it happened, and whether the person had safety and support afterward.
A practical way to understand risk is to ask one question: what was the substance doing for the person? In many cases, it was helping them sleep, blunt fear, slow racing thoughts, soften shame, or create a brief sense of distance from painful memories. That does not make substance use safe. It does explain why the two conditions so often appear together.
Women and interpersonal trauma
Among women seeking treatment for substance abuse, PTSD is estimated at 30% to 59%, according to this PubMed-listed study summary. That wide range still points in the same direction. Trauma, especially repeated interpersonal trauma such as childhood physical or sexual abuse, often sits underneath the substance use.
This helps families make sense of behavior that can otherwise look confusing. A woman may seem highly capable at work or at home while privately relying on alcohol, sedatives, or other drugs to quiet nightmares, tension, startle reactions, or emotional flooding. The outside can look organized while the inside feels like a fire alarm that never fully shuts off.
Interpersonal trauma also changes trust. If the people who were supposed to provide safety became the source of danger, closeness itself can feel risky. Substances can start to function like a fast, predictable shortcut to relief when relationships do not feel safe enough to offer comfort.
Veterans and repeated exposure to danger
Veterans also face higher risk, as noted earlier in the article. Combat, repeated threat, injury, loss, survivor guilt, and the strain of returning to civilian routines can all keep the nervous system stuck in protection mode long after deployment ends.
For some veterans, alcohol or drugs become a way to reduce hypervigilance. For others, they dull intrusive memories, irritability, or chronic sleep problems. Families may read that pattern as withdrawal or stubbornness. Often it reflects a person trying to shut off an alarm system that still acts as if danger is nearby.
The self-medication cycle can become especially strong when a substance seems to solve a specific problem quickly. If drinking leads to a few hours of sleep, or a drug briefly quiets constant scanning for danger, the brain learns that relief is available right now. Later costs, such as dependence, conflict, and worsening mood, usually arrive after that short-term relief has already reinforced the habit.
Treatment works better when it asks, “What problem was the substance solving?” before it asks the person to give it up.
Adolescents and early coping patterns
Adolescents need close attention because trauma can shape coping habits while the brain is still developing. Earlier in the article, research noted that teens with PTSD face much higher odds of alcohol, marijuana, and other drug problems than teens without PTSD.
That finding fits what clinicians often see. A traumatized teen may not say, “I am having trauma symptoms.” They may say they cannot sleep, cannot stop thinking, feel angry all the time, want to be left alone, or need something to calm down. If substances enter that picture early, the brain can start pairing distress with immediate chemical relief before healthier skills have had time to take root.
Adults sometimes miss these signs because adolescent PTSD does not always look like fear. It can look like defiance, risk-taking, emotional numbness, school problems, or sudden changes in friend groups. The behavior is still a clue.
Common risk pathways include:
- Repeated trauma exposure, which trains the body to stay on guard
- Early use for relief, where alcohol or drugs become a coping tool instead of simple experimentation
- Isolation and secrecy, which make it harder for supportive adults to notice what is happening
- Misread PTSD symptoms, where trauma reactions are labeled as attitude problems or bad choices
Once you see the pattern, the co-occurrence makes more sense. The person is not making random harmful decisions. They are often trying to manage overwhelming internal states with the tools they found first. That is also why integrated treatment matters so much. Real recovery usually begins when care addresses both the trauma driving the distress and the substance use that grew around it.
Why Co-Occurring Disorders Complicate Recovery
Treating PTSD and substance use separately sounds neat on paper. In practice, it often breaks down. If trauma remains untreated, the person keeps living with the very triggers that drive the urge to use. If substance use remains active and severe, it can interfere with sleep, concentration, and emotional steadiness, which makes trauma treatment harder to tolerate and apply.
Why treating one problem at a time often falls short
The old model often told people to get fully sober first and only then address trauma. That message can leave people feeling like they must somehow endure panic, nightmares, grief, and hypervigilance with their main coping tool removed before they're given trauma help. Many can't sustain that.
The complication isn't only clinical. It's personal. A person may stop using for a short period, then get hit by a trauma reminder and relapse quickly because no one helped them build another response. Families then assume the person “wasn't ready,” when the deeper problem may have been incomplete care.
What integrated care changes
Integrated care works from a different assumption. It assumes both conditions belong in the room from day one. That means screening for trauma in addiction treatment, talking openly about substance use in trauma treatment, and helping the person understand the links between triggers, cravings, emotions, sleep, and avoidance.
A gender-responsive lens matters too. According to this EBSCO research overview on PTSD and addiction, women with PTSD often use substances to self-medicate hyperarousal and emotional dysregulation more than men, and integrated trauma-SUD therapies show greater retention and symptom reduction in female cohorts, yet protocols still rarely differentiate by gender.
That matters because “integrated” shouldn't mean generic. The treatment plan should match the person's trauma history, substance pattern, safety needs, and real-world stressors.
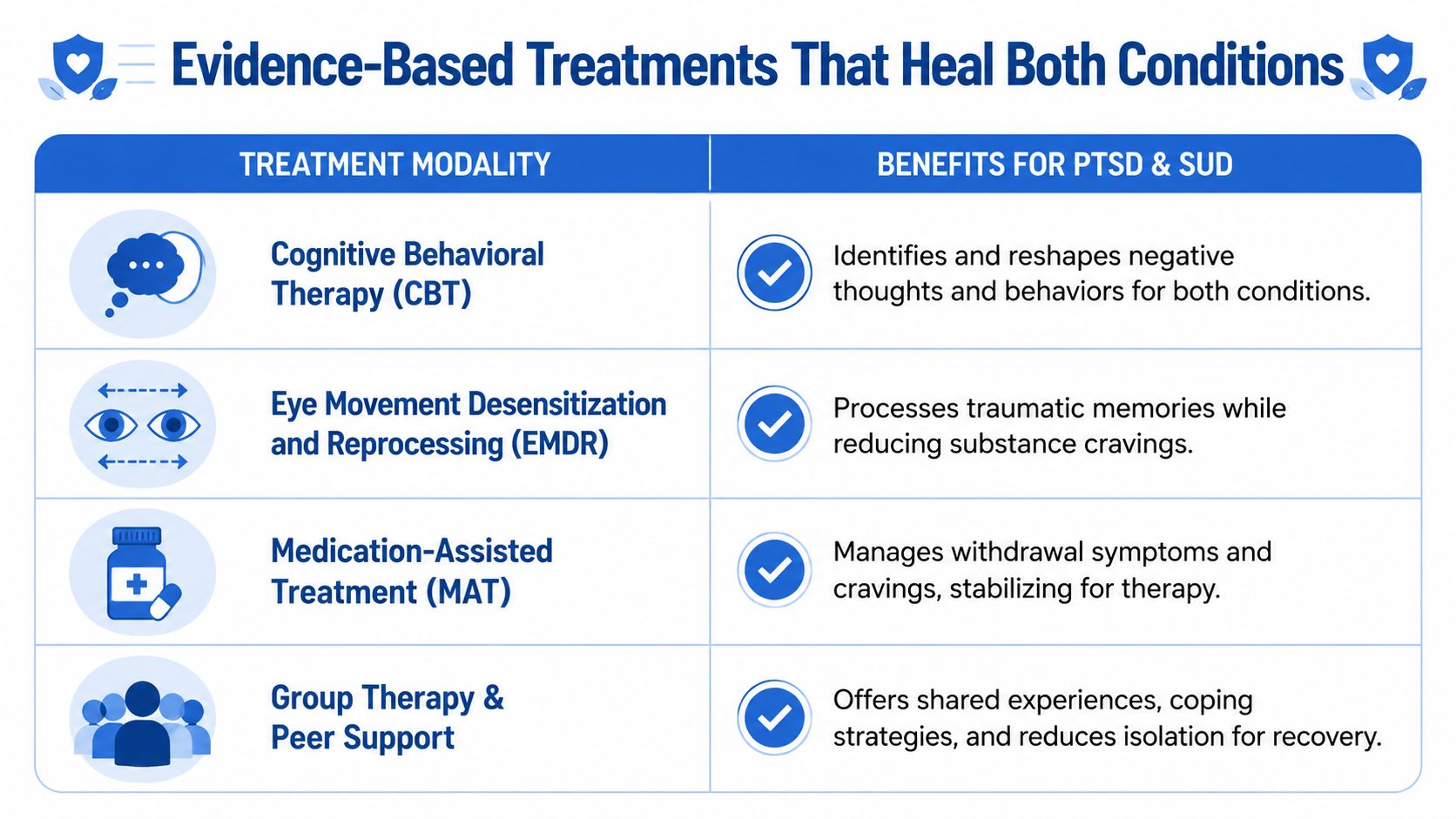
Evidence-Based Treatments That Heal Both Conditions
Healing usually works best when treatment addresses the reason a person keeps reaching for a substance, not just the substance itself. In PTSD and addiction, that reason is often straightforward even if it feels painful. Alcohol, opioids, stimulants, or marijuana may start to function like an emergency off-switch for panic, numbness, shame, nightmares, or a body that never seems to settle. Effective treatment helps a person build safer ways to regulate those states while also treating the trauma that keeps reactivating them.
Building enough stability for therapy to work
The first phase often focuses on steadiness. A person who is exhausted, withdrawing, sleeping two hours a night, and reacting to every trigger is trying to heal while their alarm system is blaring. Therapy is much easier to absorb once that alarm comes down a few notches.
Stabilization may include medically supervised detox, medications that reduce cravings or support mood and sleep, a predictable daily routine, and early coping skills for urges and flashbacks. The point is to help the brain and body stop living minute to minute.
Common goals in this phase include:
- Safer withdrawal management with monitoring and medical support
- Medication-Assisted Treatment when appropriate to reduce cravings and lower the risk of quick relapse
- Better daily regulation through food, hydration, sleep, movement, and medication adherence
- Trigger and craving tracking so the person can see the chain from reminder, to emotion, to urge, to use
That chain matters. Once people can spot it, they are no longer guessing.
Trauma-focused therapies that also support recovery
Families often worry that trauma therapy means reopening wounds too quickly. Good care is more deliberate than that. It works like physical therapy after an injury. You do not ignore the injured area forever, but you also do not push it without preparation.
Several therapies have strong support for PTSD, and they can be used as part of integrated care for people with substance use disorders:
| Therapy | What it focuses on | What a patient might experience |
|---|---|---|
| Cognitive Processing Therapy (CPT) | Trauma-related beliefs about guilt, trust, safety, power, and self-worth | Structured sessions that identify and revise stuck points after trauma |
| Prolonged Exposure (PE) | Fear, avoidance, and the habits that keep trauma symptoms active | Gradual practice approaching memories and situations that have come to feel dangerous |
| EMDR | Reprocessing distressing memories in a structured, therapist-guided format | Focused attention on traumatic memories while using bilateral stimulation |
CPT is often helpful when trauma has changed the way a person interprets everything around them. A survivor may start living by rules such as “I caused this,” “No one can be trusted,” or “If I feel anything, I will fall apart.” CPT helps test those beliefs carefully and replace them with thoughts that are more accurate and less punishing. Clinicians who want a practical overview of the model can use this guide for CPT clinicians.
PE helps reduce the power of avoidance. That matters because avoidance often feeds both PTSD and substance use. If a memory, place, smell, conflict, or body sensation feels unbearable, using can start to look like the fastest exit. PE teaches the person, with support and pacing, that distress can rise and fall without needing a substance to shut it down.
EMDR can be a good fit for some patients as well. Some find it easier to tolerate because the structure feels contained, though fit depends on the person's symptoms, stability, substance pattern, and clinical assessment.
Treating both conditions at the same time
A common fear is that trauma work will trigger more use. Research does not support treating PTSD as off-limits until long after sobriety is established. The VA and National Center for PTSD overview of co-occurring PTSD and substance use disorder explains that trauma-focused psychotherapies can be offered to patients with both conditions and should not be routinely withheld because of substance use alone.
The better question is not, “Should trauma ever be treated during addiction care?” The better question is, “What level of support does this person need to do trauma work safely and stay engaged?”
That leads to practical treatment planning. Some people begin with more focus on withdrawal, sleep, cravings, and basic coping. Others are ready for trauma processing sooner. In both cases, the plan should connect the same moving parts: trauma reminders, body reactions, thoughts, cravings, behavior, and relapse risk.
Effective care often includes:
- Individual therapy to address trauma symptoms and the self-medication cycle directly
- Group therapy so patients can practice skills, reduce shame, and hear that their pattern is understandable
- Medication support when indicated for cravings, mood symptoms, or sleep disruption
- Family education so loved ones can respond to triggers and relapse warning signs with more clarity
- Aftercare planning that prepares for the test, returning to daily life where reminders and urges often show up fast
Recovery tends to strengthen when treatment helps a person answer two questions at once: “What happened to me?” and “What do I do instead of using when it hurts?”
How Addiction Resource Center Provides Integrated Care
Good integrated care depends on whether a program can treat the whole picture, not just one symptom at a time. In Yuba City, that means having medical support, addiction treatment, mental health care, and practical follow-through in one coordinated plan instead of scattering them across separate providers.
One plan instead of fragmented treatment
Addiction Resource Center LLC describes a model built for adults with substance use disorders and co-occurring mental health needs. Its services include medically supervised detox with Medication-Assisted Treatment, residential rehabilitation through Ona Treatment Center in Browns Valley, and an Intensive Outpatient Program offered both in person and through telehealth.
What stands out is the team structure. Care is delivered by a medical doctor, registered nurse, licensed counselors including CADCs, a licensed marriage and family therapist, and recovery mentors. That matters because trauma and addiction treatment often fall apart when each provider works in isolation.
A coordinated team can help with needs such as:
- Withdrawal and medication support when the body needs stabilization
- Therapy for trauma and substance use under one treatment direction
- Relapse prevention planning that includes triggers, warning signs, and family dynamics
- Mentor support and accountability for the hours outside formal sessions
Access points that lower barriers
People delay treatment for practical reasons as much as emotional ones. They may need telehealth, a lower level of care after detox, privacy, family guidance, or help understanding insurance. A program that offers several entry points can reduce that friction.
Addiction Resource Center LLC also notes experience with major insurance plans and TRICARE, which can matter for veterans and military families seeking care close to home. For people who need a clearer picture of how digital tools can support coordination, communication, and patient experience in care settings, this overview of Ekipa AI for digital health companies offers a useful look at the broader technology side of healthcare operations.
The best local program isn't the one with the most jargon. It's the one that can meet the patient where they are, keep care connected, and make the next step feel possible.
A down-to-earth environment also matters more than many people realize. Patients with PTSD often scan for threat, judgment, and loss of control. Privacy, predictability, and respectful communication aren't extras. They help determine whether someone stays in treatment long enough to benefit from it.
Your Next Steps to Begin Healing in Yuba City
If PTSD and substance use are tangled together in your life, the next step doesn't have to be dramatic. It just has to be clear.
Start with a simple conversation. Call or text a treatment provider and say what is happening right now, even if you don't have the perfect words. You can say, “I'm drinking because my anxiety is out of control,” or “My loved one has trauma and uses to cope.” That's enough to begin.
A practical checklist can help:
- Reach out confidentially. Ask for a private conversation about symptoms, substance use, safety concerns, and treatment options.
- Verify insurance early. If you have private insurance or TRICARE, ask what level of care may be covered.
- Ask about the right starting point. Some people need detox first. Others may fit outpatient or telehealth support.
- Schedule a tour or intake. Seeing the setting can lower fear and make treatment feel more real.
- Bring one support person if that helps. Many people make first contact more easily when they aren't doing it alone.
Healing usually starts before confidence shows up. Many people reach out while scared, ashamed, ambivalent, or exhausted. That's normal. You don't have to feel fully ready to take the next step.
If you're looking for compassionate local help, Addiction Resource Center LLC in Yuba City offers medically supervised detox, MAT, residential treatment through its partner program, in-person and telehealth IOP, and support for co-occurring mental health needs. You can call or text 530-625-7910 any time for a free, confidential conversation, ask about insurance or TRICARE, or schedule a no-obligation tour at 1002 Live Oak Blvd., Suite A, Yuba City, CA.