You may be sitting with a phone in your hand, staring at a treatment website, trying to figure out why the same pattern keeps happening. Your loved one stops drinking or using for a short time, seems better for a few days, then the panic, anger, depression, sleeplessness, or paranoia comes rushing back. Soon the …
You may be sitting with a phone in your hand, staring at a treatment website, trying to figure out why the same pattern keeps happening. Your loved one stops drinking or using for a short time, seems better for a few days, then the panic, anger, depression, sleeplessness, or paranoia comes rushing back. Soon the substance use returns too. It can feel like you're watching two fires feed each other.
Families often blame the wrong thing. They think the problem is only alcohol, only pills, only meth, only weed. Or they think the problem is only anxiety, only depression, only trauma. In many cases, it's both at the same time. When that happens, treatment has to make room for both problems from the start.
The clinical term is co-occurring disorders, also called dual diagnosis. It means a person has a substance use disorder and a mental health disorder that affect each other in real life, not just on paper. If you're trying to understand what care looks like, this guide walks through it in plain language, step by step, so you can see what help should involve and what questions to ask next.
Table of Contents
- When It Is More Than Just Addiction
- What Is a Dual Diagnosis or Co-Occurring Disorder
- Why Integrated Treatment Is the Gold Standard
- Navigating the Levels of Care
- What Happens During Treatment
- How to Access and Pay for Care
- Your Journey to Recovery Starts Here
When It Is More Than Just Addiction
A family member might say, “If he could just stop using, everything would calm down.” Sometimes that's partly true. But sometimes the drinking or drug use has been covering up something deeper, or making something deeper much worse.
Take a common situation. A person drinks heavily at night because they can't shut off constant worry. They finally stop drinking, but now they're flooded with anxiety, they can't sleep, and they feel like they're crawling out of their skin. Everyone around them says, “See, this is why you need to stay sober.” They're trying. But without treatment for the anxiety itself, sobriety can feel unbearable.
Another person might use stimulants for bursts of energy and confidence, then crash into depression. A third may rely on opioids after trauma because numbing out feels safer than feeling anything. In each case, the substance use and the mental health symptoms become tangled together. One keeps triggering the other.
Some relapses aren't a sign that treatment failed. They can be a sign that treatment was too narrow.
That's the point where families get exhausted and confused. They've tried detox, promises, ultimatums, even short periods of counseling. Yet the cycle keeps repeating because no one has treated the whole picture.
Dual diagnosis addiction treatment is meant for that whole picture. It doesn't ask a person to fix one major problem while the other is ignored. It recognizes that both conditions need attention, and that recovery becomes more stable when care is coordinated instead of fragmented.
What Is a Dual Diagnosis or Co-Occurring Disorder
A dual diagnosis means a person is living with both a mental health disorder and a substance use disorder. These conditions can appear together in many ways. Sometimes a person uses substances to dull emotional pain. Sometimes heavy substance use makes mental health symptoms more intense. Often it's hard to tell which started first, and in day-to-day treatment that question usually matters less than treating both safely.
Why both problems have to be treated together
A simple way to think about it is a boat with two leaks. If you only patch one hole, the boat still takes on water. If you only scoop water out with a bucket, but the leaks stay open, the boat still sinks. That's what happens when treatment focuses only on addiction or only on mental health.

In real life, this can look like someone who stops using meth but still has untreated paranoia, or someone who begins antidepressant care but keeps drinking heavily every night. Progress on one side keeps getting undermined by the other side.
Common combinations families notice first
You don't need a clinical background to notice patterns. Families often first recognize dual diagnosis through combinations like these:
- Anxiety and alcohol. The person says alcohol is the only thing that helps them calm down.
- Depression and opioids. They seem numb, withdrawn, and trapped in a cycle of pain relief and emotional shutdown.
- PTSD and stimulants. They use substances to stay alert, avoid sleep, or push away traumatic memories.
- Bipolar symptoms and substance use. Mood swings, impulsive behavior, and drug or alcohol use start feeding each other.
- Panic symptoms and benzodiazepine misuse. Relief becomes dependence, and dependence increases fear.
If you're learning more about effective dual diagnosis care, one helpful filter is whether a program explains how both conditions are treated at the same time, not in separate silos.
Why finding the right program matters
This part surprises many families. Approximately 18% of addiction treatment programs and 9% of mental health treatment programs in the United States are classified as Dual Diagnosis Capable, according to a peer-reviewed review on dual diagnosis capability. That means many people seeking help still land in settings where one condition is addressed first and the other is postponed or handled lightly.
When a program isn't equipped for co-occurring disorders, people often hear versions of the same message: get sober first, then deal with the depression. Or stabilize the anxiety first, then address the addiction. For some people, that split approach leaves the main cycle intact.
Practical rule: If a provider can't clearly explain how mental health care and addiction care are coordinated, keep asking questions.
Why Integrated Treatment Is the Gold Standard
The strongest approach for co-occurring disorders is integrated treatment. That phrase can sound technical, but the idea is simple. One team works on both the mental health condition and the substance use disorder together, in one coordinated plan.
The older step-by-step model
Many families have already run into the older model without realizing it. A detox program says, “First get the substances out.” A counselor later says, “Now start therapy for trauma.” A psychiatrist somewhere else adjusts medication. None of these steps are wrong on their own. The problem is that the patient ends up carrying the treatment plan alone.
That creates gaps. One provider may not know what another provider is seeing. Medication decisions may ignore addiction risk. Addiction counseling may miss severe depression, mania, or trauma symptoms that are driving cravings.
This visual shows the difference between separated care and coordinated care.

What integrated care looks like in practice
Integrated Dual Disorder Treatment, often shortened to IDDT, brings together medication, therapy, education, and social support through one multidisciplinary team in one service organization, as described in this review of integrated treatment for co-occurring disorders. In plain terms, the doctor, nurse, therapist, counselor, and support staff are working from the same playbook.
That matters during detox, during medication changes, during therapy, and during relapse prevention planning. If a person starts having panic symptoms, the team doesn't treat that as a separate side issue. If cravings spike after trauma work begins, the team adjusts the plan instead of acting surprised.
A short video can help make that integrated model easier to picture.
Why this approach matters
Research on IDDT shows an important nuance. In the review above, 54.5% of studies showed comparable reductions in substance use outcomes between integrated and non-integrated approaches, but integrated treatment had a statistically significant advantage in improving psychiatric symptomatology. That's a key point for families. Even when substance use measures look similar, integrated care can better stabilize the mental health symptoms that often make recovery fragile.
When anxiety, depression, trauma symptoms, or psychosis remain untreated, “just stop using” isn't a complete plan.
This is why integrated care is considered the gold standard in dual diagnosis addiction treatment. It treats the person as one person, not as two separate problems handed off between systems.
Navigating the Levels of Care
For many families, treatment feels mysterious until they can see the actual path. It usually helps to think in stages rather than one big decision. A person may need detox first, then a more structured setting, then a step down into outpatient care, and later an aftercare plan that keeps recovery supported in daily life.
Step one starts with a full assessment
The first step should be a thorough assessment, not a rushed intake that only asks what substances were used. A good assessment looks at current use, withdrawal risk, mental health symptoms, medication history, safety concerns, physical health, housing stability, and family support.
Clinicians then begin answering practical questions such as:
- Is detox needed right away because stopping suddenly could be dangerous or overwhelming?
- Are psychiatric symptoms active in a way that needs immediate attention?
- Can this person safely function at home, or do they need a more protected setting?
- What level of structure fits best for work, school, parenting, legal obligations, or medical needs?
Detox when safety comes first
Detox is the stabilization stage. Its job is not to “fix everything” in a few days. Its job is to help the body and mind get through withdrawal safely while the team starts understanding what symptoms belong to withdrawal, what symptoms may be part of a mental health disorder, and what support should come next.
Medically supervised detox can also include medication-assisted treatment, often called MAT, when appropriate. That may mean medication to reduce withdrawal distress, lower cravings, or support stability while psychiatric care is being coordinated.
What families should know: The end of detox is the start of treatment, not the end of treatment.
Residential rehab for a protected reset
Some people need a period of living in a treatment setting away from daily triggers. Residential rehab can help when the home environment is chaotic, relapse risk is high, or the person needs round-the-clock support while building basic routines again.
In a residential setting, the day is structured. There are therapy sessions, groups, medication monitoring, meals, rest, and recovery-focused routines. For someone whose life has become disorganized by both addiction and mental health symptoms, that structure can create breathing room.
Residential care is often a strong fit when a person keeps trying to recover at home and keeps getting pulled back into the same pattern.
IOP for structure without full-time residence
An Intensive Outpatient Program, or IOP, gives substantial treatment while allowing the person to live at home. This can work well for someone who is medically stable, has a safer living environment, or needs to keep some connection to work, school, or family responsibilities.
IOP isn't “less serious” care. For many people, it's the most realistic way to sustain treatment in real life. It allows them to practice coping skills where triggers occur, while still receiving regular support. Telehealth options can make IOP more accessible for people who can't easily attend every service in person.
Comparing Treatment Settings Residential vs IOP
| Feature | Residential Rehab | Intensive Outpatient Program (IOP) |
|---|---|---|
| Living arrangement | Lives on site in a structured environment | Lives at home or in supportive housing |
| Daily structure | High structure throughout the day | Scheduled treatment sessions during the week |
| Best fit | Higher relapse risk, unstable environment, need for close supervision | Medically stable, able to function outside treatment hours |
| Exposure to triggers | Lower immediate exposure while skills are built | Ongoing real-world exposure with clinical support |
| Family logistics | Time away from home responsibilities | Greater flexibility for work, school, or parenting |
| Clinical focus | Stabilization, routine, immersive therapy | Skill practice, accountability, continued symptom management |
A person may move through more than one level of care. That isn't a setback. It's often the right way to match treatment intensity to what's needed at each stage.
What Happens During Treatment
Once a family understands the level of care, the next question is usually more personal: what will my loved one do every day? The answer is that treatment works through repeated, practical interventions. It's not only talking. It's not only medication. It's a blend of supports that help the person stabilize, understand patterns, and practice different responses.
A treatment day usually includes several layers of care
Most strong dual diagnosis addiction treatment plans combine several elements rather than relying on one tool.
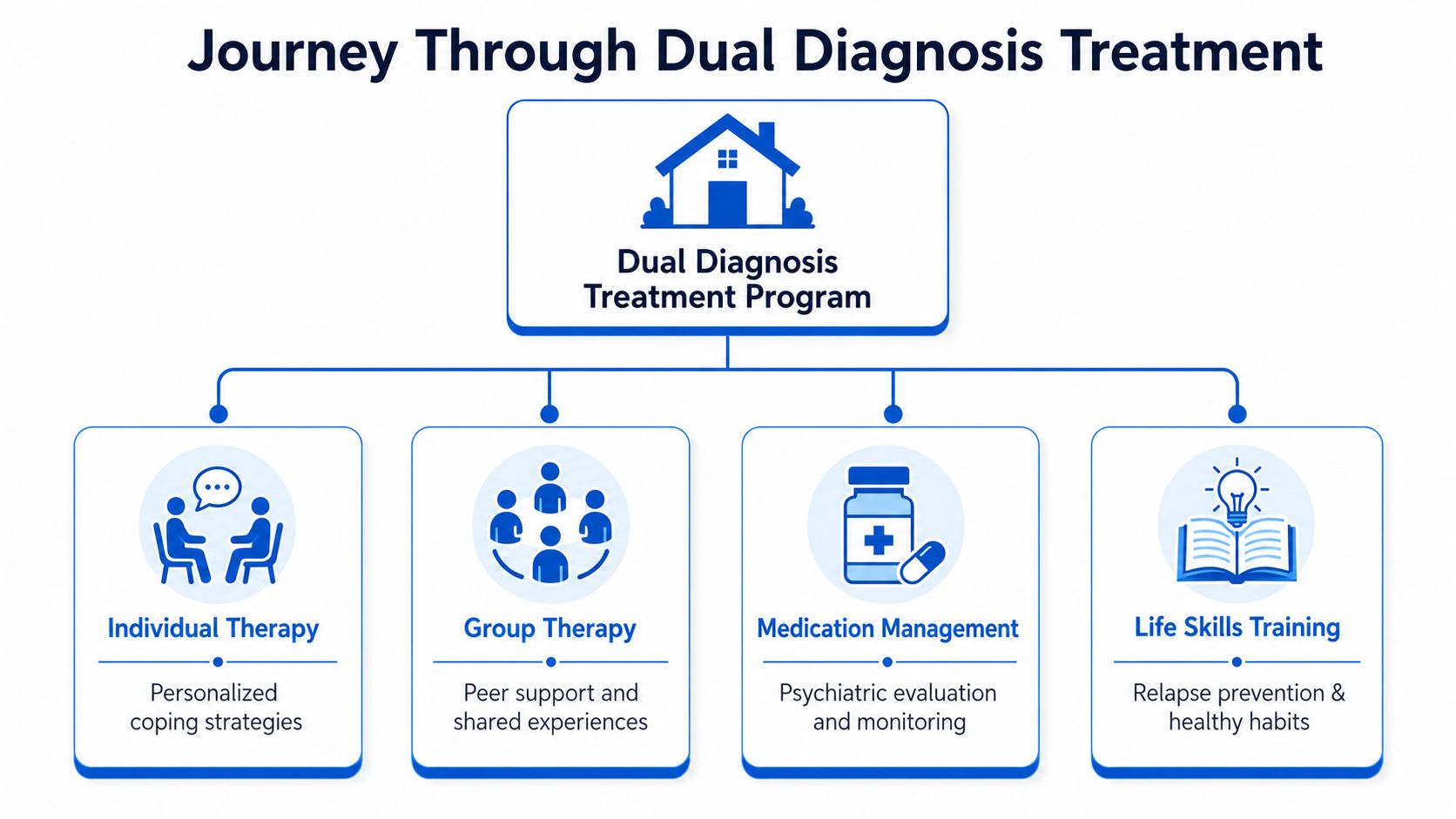
A treatment plan may include:
- Individual therapy to sort out triggers, trauma history, distorted thinking, and relapse patterns.
- Group therapy to reduce isolation and let people practice honesty, boundaries, and peer support.
- Medication management for cravings, withdrawal support, mood symptoms, sleep issues, anxiety, or other psychiatric concerns.
- Psychoeducation so the person understands what their symptoms mean and what tends to make them worse.
- Life skills work such as planning routines, handling stress, managing conflict, and building sober structure.
Why medication can be part of recovery
Some families worry that medication means the person isn't “really” recovering. In dual diagnosis care, medication can be one part of a carefully supervised plan. MAT may help with cravings or withdrawal. Psychiatric medication may help with depression, anxiety, mood instability, or other symptoms that keep pulling the person back toward substance use.
The key is fit. Medication should be chosen and monitored in the context of the person's whole recovery picture, not added casually.
The integrated clinical reality is that dual diagnosis treatment often combines behavioral therapy, medication, and support groups at the same time, as described in this discussion of how dual diagnosis treatment works. That source also notes an important nuance: about 50% of people with co-occurring disorders respond well to combined treatment, while others may need a more individualized, sequential, or augmented approach.
Therapy teaches skills, not just insight
People often picture therapy as sitting in a chair talking about childhood. That can be part of it, but effective treatment is usually much more active.
A therapist using CBT helps the person notice links between thoughts, feelings, and behavior. For example, “I can't calm down unless I drink” becomes something the patient learns to test, challenge, and replace. A therapist using DBT may focus more on distress tolerance, emotion regulation, and getting through intense moments without acting impulsively.
That's why one-size-fits-all treatment often falls short. Some people need detox plus MAT and outpatient therapy. Some need residential care first. Some do well with telehealth as part of outpatient treatment because it keeps them engaged when transportation, work schedules, or childcare make in-person care harder.
Treatment should adapt to the person. The person shouldn't have to force their life into one rigid model.
Family work helps recovery hold
Addiction and mental health symptoms affect the whole household. Families may feel angry, frightened, exhausted, guilty, or all of those at once. Family therapy can help everyone learn healthier communication, clearer boundaries, and a more realistic picture of what support looks like.
That doesn't mean family members caused the disorder. It means recovery tends to hold better when the home environment becomes steadier, less reactive, and more informed.
How to Access and Pay for Care
When a family is in crisis, practical details matter. You need to know what to ask, how insurance works, and how to start without getting bounced around.

Questions to ask before choosing a program
Call the provider and listen closely to how they answer. Clear answers usually signal organized care.
- How do you treat addiction and mental health together rather than separately?
- Who is on the treatment team for medication, therapy, and recovery support?
- Do you offer medically supervised detox if withdrawal may be unsafe?
- What levels of care are available if the person needs more or less structure over time?
- How is family involved when the patient agrees?
- What happens after the first stage of treatment so the person doesn't leave without a next step?
What to ask about insurance and admission
Financial fear stops many people from calling. It shouldn't. A quick insurance verification can tell you a lot before admission decisions are made.
Ask questions like these:
- Do you accept my insurance plan and can you verify benefits confidentially?
- Do you work with TRICARE if the patient is a veteran or part of a military family?
- What should we bring for intake, including ID, insurance card, and medication list?
- How soon can an assessment happen if the situation feels urgent?
Local access details if you are ready to call
For people in Yuba City and nearby parts of Northern California, local access can make the first step feel more manageable. Addiction Resource Center LLC offers medically supervised detox with MAT, residential rehabilitation through Ona Treatment Center in Browns Valley, intensive outpatient care in person and via telehealth, and support for co-occurring mental health needs.
Most major insurance plans are accepted, and TRICARE beneficiaries are welcome. The center is located at 1002 Live Oak Blvd., Suite A, Yuba City, CA, and the 24/7 phone and text line is 530-625-7910. If you're overwhelmed, keep the first goal simple: call, explain what's happening, and ask what level of care makes sense.
Your Journey to Recovery Starts Here
If your loved one has been caught in the loop of addiction plus anxiety, depression, trauma, or another mental health condition, there is a reason simple solutions haven't worked. The problem may be bigger than substance use alone, and the answer may need to be broader too.
That's the hopeful part. Dual diagnosis addiction treatment exists because this pattern is recognized, treatable, and common enough that families shouldn't have to guess their way through it. Good care looks at the full person, matches the level of support to the specific situation, and adjusts the plan when one approach isn't enough.
You don't need to solve everything today. You only need one clear next step. For many families, that step is a confidential conversation with someone who can help sort out whether detox, residential rehab, MAT, or outpatient support fits best.
If you're ready to talk through options for yourself or someone you love, Addiction Resource Center LLC offers compassionate guidance, confidential insurance verification, and a full continuum of care in Yuba City. A simple phone call or text can help you understand what comes next, whether you need detox, outpatient support, residential placement, or just clear direction during a hard moment.