Most rehab programs are built around 30, 60, or 90 days, but the right answer is personal, not universal. For some people, detox lasts only a few days, while others do best with 90 days or more, especially if they've relapsed before, have co-occurring mental health needs, or need a longer step-down plan. If you're …

Most rehab programs are built around 30, 60, or 90 days, but the right answer is personal, not universal. For some people, detox lasts only a few days, while others do best with 90 days or more, especially if they've relapsed before, have co-occurring mental health needs, or need a longer step-down plan.
If you're searching this late at night, refreshing tabs, comparing centers, and wondering how long life is supposed to stop so recovery can start, you're not alone. This question usually isn't just about a calendar. It's about work, family, money, fear, and the quiet hope that this time might finally stick.
A lot of people call treatment providers wanting one simple number. They ask, “Is rehab 30 days?” Sometimes the honest answer is yes. Sometimes it's 60. Often it's 90. And for many people, especially those with a long history of substance use or repeated relapse, the most effective path isn't a single stay at all. It's a sequence of care that gives the brain, body, and daily routines time to change.
That's the part many articles skip. If someone needs longer treatment after one or more relapses, that doesn't mean they failed treatment. It usually means the treatment plan needs to match the reality of the illness more closely. Recovery is not a race to discharge. It's a plan for staying well after discharge.
Table of Contents
- The Search for a Simple Answer to a Complex Question
- Standard Rehab Timelines A Breakdown by Program Type
- Five Key Factors That Determine Your Treatment Length
- What to Expect The Three Phases of Rehabilitation
- Why 90 Days or More Is the Gold Standard for Lasting Recovery
- How to Find the Right Level of Care at Addiction Resource Center
The Search for a Simple Answer to a Complex Question
A man in his forties calls after trying to stop drinking on his own. He wants to know if he can “get this handled in 30 days” because he's worried about work. A mother asks about her adult daughter and lowers her voice when she says there's been more than one relapse. A young veteran wants to know whether treatment means disappearing for months or whether there's a way to build care around real life.
Those are very different situations, even though all three are asking the same thing. How long does rehab take? The answer depends on what has to happen during treatment, not just on what sounds manageable on the front end.
Some people need medical support first because withdrawal could be dangerous. Some need residential care because home is chaotic or full of triggers. Some are stable enough for outpatient treatment but still need frequent therapy, accountability, and medication support. And some need a longer runway because each previous attempt showed that a short reset wasn't enough.
Practical rule: Don't ask only, “How fast can this be done?” Ask, “What level of care gives me the best chance of staying sober after I leave?”
That shift matters. A shorter timeline can feel emotionally easier to accept. But if the plan ends before cravings, routines, mental health symptoms, and relapse triggers are addressed, the calendar may look efficient while the outcome feels fragile.
People often feel ashamed when they learn they may need more than a standard 30-day stay. They shouldn't. A longer recommendation usually reflects clinical judgment, not personal weakness. If someone has relapsed before, needs medication-assisted treatment, or is dealing with both addiction and mental health symptoms, more time often means a more realistic plan.
Standard Rehab Timelines A Breakdown by Program Type
Why program names can feel confusing
A lot of people call every form of addiction treatment "rehab," but treatment usually happens in stages. One person may need detox and then residential care. Another may skip inpatient treatment and start in an outpatient program with therapy, medication, and regular check-ins.
That is why the timeline can sound inconsistent at first. Program names describe the level of support, the setting, and how many hours of care a person receives each week. They are less like different brands of rehab and more like different rungs on a ladder. As a person becomes safer, steadier, and more able to practice recovery in daily life, the level of care often steps down.
Federal treatment planning guidance from the Substance Abuse and Mental Health Services Administration explains that care should match the person's clinical needs and can change over time as those needs change. That helps explain why two people with the same substance of choice may still get very different recommendations.
A simple comparison of treatment levels
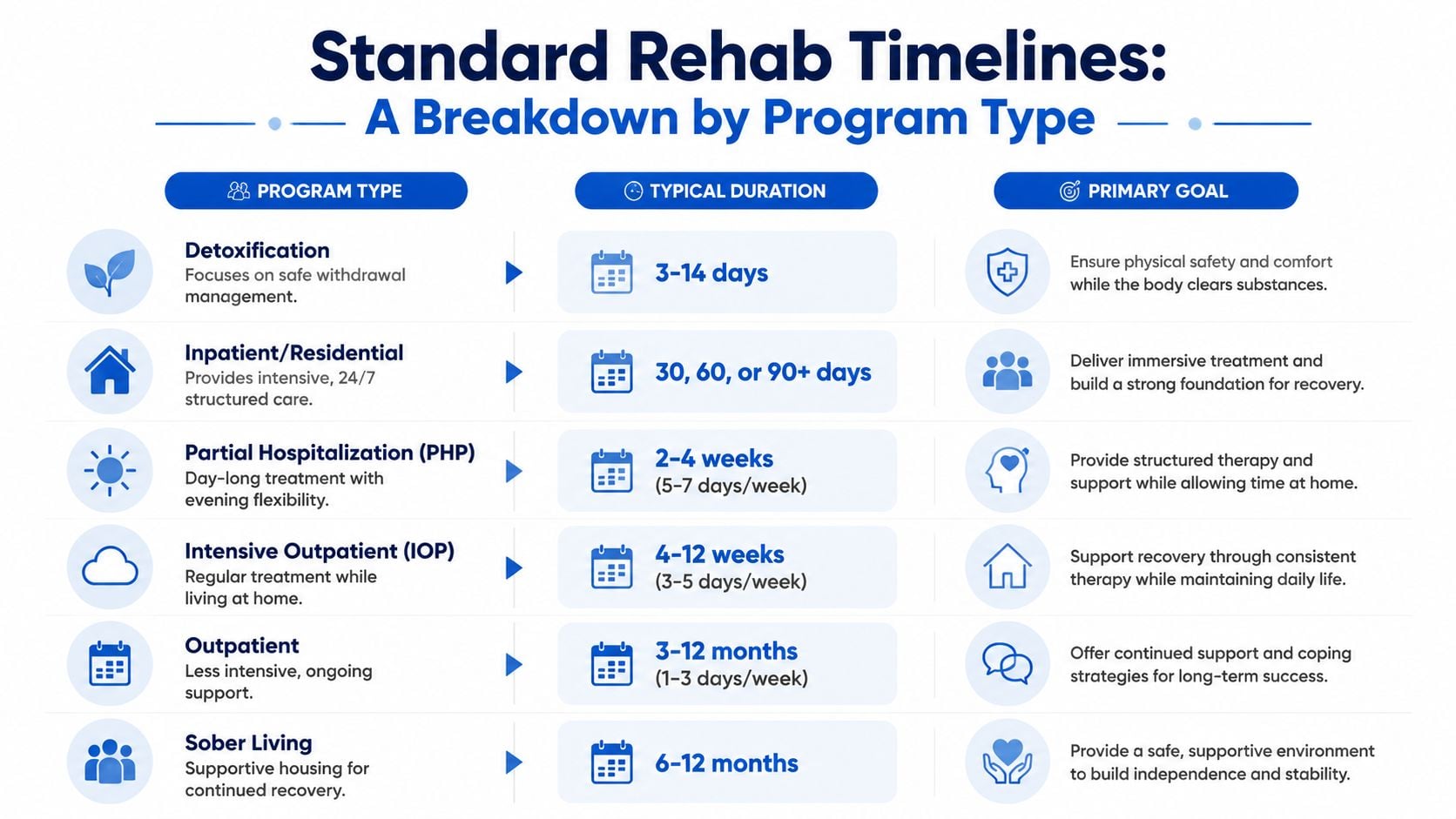
| Program Type | Typical Duration | Best For |
|---|---|---|
| Detox | A few days to about two weeks | People who need safe withdrawal management and medical stabilization |
| Inpatient or Residential | 30, 60, or 90+ days | People who need 24/7 structure, distance from triggers, and daily therapy |
| Partial Hospitalization Program | Several weeks | People who need a high level of support without overnight care |
| Intensive Outpatient Program | Several weeks to a few months | People who are stable enough to live at home while attending treatment multiple times each week |
| Outpatient | Ongoing, often months | People stepping down from higher levels of care or needing continued support |
| Medication-Assisted Treatment | Often long term | People recovering from opioid or alcohol use who benefit from medication plus counseling |
| Sober Living | Often several months | People who need a supportive bridge between treatment and independent living |
A few of these labels deserve plain-English explanation.
- Detox focuses on getting through withdrawal safely. It is the opening chapter, not the whole book.
- Residential care means recovery is the person's main job for a period of time, with structure from morning to night.
- PHP and IOP provide intensive therapy and accountability while the person lives at home or in supportive housing.
- Outpatient care and aftercare help someone keep practicing recovery once the most acute phase has passed.
- Medication-assisted treatment can continue much longer than other services because medications for opioid or alcohol use disorder are often part of long-term relapse prevention, not a short-term reset.
How the timeline often unfolds in real life
A real treatment plan often works like a cast after a broken bone. At first, support may need to be firm and protective. Later, the goal shifts to rebuilding strength while the person starts using that strength in everyday life.
So the timeline often looks like a sequence, not a single block on a calendar. A person might complete detox, spend time in residential treatment, move into PHP or IOP, and continue with outpatient therapy, medication management, recovery meetings, or sober living. Each step serves a different purpose.
This matters for people with a history of relapse. If someone has tried shorter care several times and keeps returning to use, a longer timeline is not a sign that they failed treatment. It often means the treatment team is responding to what previous attempts already taught them. In plain terms, a short stay may have helped with crisis stabilization but not given enough time to build new routines, treat mental health symptoms, repair sleep, practice coping skills, and stay supported through the risky transition back to daily life.
The National Institute on Drug Abuse notes in its principles of effective treatment that people need adequate time in treatment for it to be effective, and that participation for less than 90 days is often of limited effectiveness for residential or outpatient treatment. That does not mean every person needs the exact same schedule. It means recovery usually has a better chance when the plan lasts long enough to work.
A discharge date is not the finish line. It is one checkpoint in a longer recovery process.
Cost also shapes what people believe is possible, which is why families sometimes ask for the shortest option first. That reaction is understandable. Still, the least expensive timeline on paper can become the more costly one in real life if it leads to repeated relapse, repeated admissions, missed work, medical complications, or another crisis. A well-matched level of care is often the more practical choice over time.
The question "how long does rehab take" sounds like it should have one clean answer. Usually it has several. The right timeline depends on where treatment starts, how much structure is needed, and whether the goal is short-term interruption of use or lasting recovery with enough support to make the change stick.
Five Key Factors That Determine Your Treatment Length
The clinical factors that shape the timeline
A person calls expecting a simple answer. “Do I need 30 days, 60 days, or longer?” The honest answer is that a treatment team is not choosing a number first. They are looking at what will give this particular person a real chance to stabilize, practice new skills, and stay safe after discharge.
Recovery planning works a lot like setting a broken bone. A small fracture and a complicated break do not heal on the same schedule, even if both injuries matter. Addiction treatment follows that same logic. The timeline changes based on what the person is carrying into care, what risks show up during treatment, and what support will be waiting on the outside.
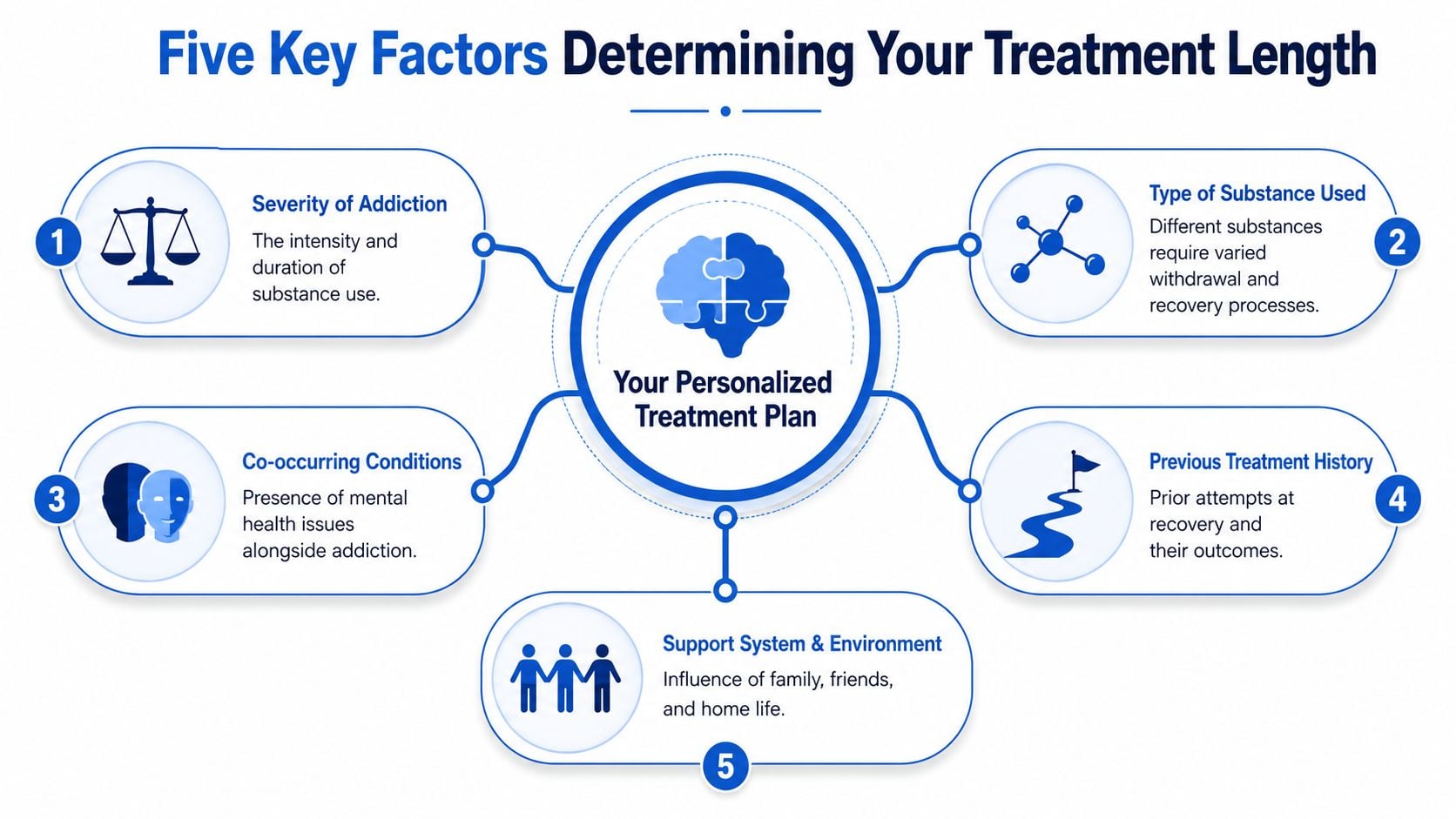
Five factors usually shape that recommendation.
1. Severity and duration of substance use
Someone who has been using heavily for a long time often needs a longer runway. The brain and body may need more time to settle, sleep may take longer to normalize, and the person may need more repetition before coping skills feel usable in real life.
2. The substance used and the withdrawal pattern
Alcohol, opioids, benzodiazepines, stimulants, and polysubstance use do not create the same treatment picture. Some substances bring higher medical risk in withdrawal. Others leave behind intense cravings, depression, or exhaustion that can make early recovery feel shaky even after detox is over.
3. Mental health needs
Anxiety, depression, trauma, bipolar disorder, and other mental health concerns can lengthen treatment because both conditions need attention at the same time. If one part is treated and the other is ignored, progress often slips. Integrated care takes time, but it usually gives people a stronger foundation.
4. Medical and medication needs
Some people need close monitoring, medication-assisted treatment, psychiatric follow-up, sleep support, or help managing chronic health conditions. That does not mean they are doing worse. It means the plan has more moving parts, and each part needs enough time to work safely.
5. The recovery environment after treatment
Discharge planning matters because people do not recover in a vacuum. A stable home, reliable transportation, family support, and follow-up care can make outpatient treatment more realistic. An unsafe home, conflict, homelessness, or constant exposure to substance use often means a longer or more structured level of care is the safer choice. For some families, learning what is transitional care also helps them understand why a step-down setting can protect progress during that vulnerable period between intensive treatment and fully independent living.
Why relapse history changes the recommendation
This factor deserves special attention because it carries so much shame.
If someone has relapsed before, a longer recommendation is not a sign that they failed treatment. It usually means the earlier dose of treatment was not enough for the situation. A short stay may have helped them stop using, but it may not have given enough time for trauma work, medication adjustments, family repair, relapse prevention practice, or a stable housing plan.
That is why relapse history often changes the timeline. Clinicians are not punishing the person for needing more help. They are using the person's actual history to choose a plan with better odds.
A helpful way to view this is to compare treatment length to physical therapy after reinjury. If a knee gives out again, the answer is often more support, more practice, and a longer recovery plan, not blame. Addiction care works in much the same way. Repeated relapse can point to unresolved triggers, untreated mental health symptoms, an unstable home environment, or a level of care that ended before new habits had time to stick.
Longer treatment can be an effective clinical strategy, especially for people who have tried to “get better fast” before and then found themselves back in the same cycle. More time can allow the person to move beyond crisis management and build something steadier: insight, routine, support, and a discharge plan that fits real life.
Life demands still matter. Work, childcare, school, and finances affect what is possible. A good treatment team takes those pressures seriously while also being honest about risk. The goal is not to keep someone in care longer than needed. The goal is to match the timeline to what gives recovery a fair chance.
What to Expect The Three Phases of Rehabilitation

A family often calls with one quiet fear behind all the practical questions: “What happens after admission, and how do we know if enough time has passed?” That question matters even more when someone has been through treatment before. If a person has a relapse history, the answer is often not “repeat the same short stay.” It may mean giving each phase more time so the work can hold under real-life stress.
Treatment usually unfolds in three broad phases. The phases are simple to name, but they are not a conveyor belt. People move through them at different speeds based on withdrawal risk, mental health needs, medical stability, motivation, and what has or has not worked in prior treatment.
Phase one stabilization and detox
The first days are usually focused on getting the person medically and emotionally steady. Staff gather history, review substance use patterns, check for withdrawal risk, and look at practical concerns such as medications, sleep, nutrition, and safety.
For some people, this phase is short. For others, it takes longer because the body and brain need more time to settle. Opioids, alcohol, benzodiazepines, stimulant crashes, or co-occurring anxiety and depression can all change what stabilization looks like. A person with prior relapses may also need closer observation at the start, especially if earlier treatment ended before withdrawal, cravings, or psychiatric symptoms were fully addressed.
This phase can feel uncomfortable and disorienting. Sleep may be poor. Emotions may feel close to the surface. Relief and fear often show up together.
Phase two therapy and skill building
Once the immediate crisis eases, the work gets deeper. This is the phase where treatment begins to answer the harder question: why does substance use keep returning, even when the person wants life to change?
Recovery work here often includes individual counseling, group therapy, education about addiction, relapse prevention planning, family sessions, and medication review when appropriate. The goal is not only to stop using. It is to help the person recognize patterns early enough to interrupt them.
Rehab works a lot like rebuilding strength after an injury. Early care helps with immediate stabilization, but repeated practice is what helps the body hold up under pressure. In the same way, people in treatment often need repetition to turn insight into behavior.
Common parts of this middle phase include:
- Individual therapy: Examining trauma, grief, shame, anger, thought patterns, and mental health symptoms tied to substance use.
- Group sessions: Hearing familiar stories, practicing honesty, and reducing the isolation that often fuels relapse.
- Practical recovery skills: Managing cravings, setting boundaries, improving sleep, handling conflict, and preparing for high-risk situations.
- Family work: Clearing up confusion, setting expectations, and helping the home environment support recovery instead of accidentally undermining it.
For someone with a relapse history, this phase is often where a longer timeline makes the most clinical sense. A short stay may help a person understand their triggers. Longer care gives them time to practice different responses until those responses feel more natural.
Phase three transition and aftercare planning
The final phase focuses on the handoff to everyday life. Discharge is not a finish line. It is a transfer from one level of support to the next.
That plan may include a step down to PHP, IOP, outpatient therapy, medication management, sober living, peer support, family follow-up, and a written relapse response plan. Good planning also covers practical details such as transportation, housing, work expectations, childcare, and who the person will call when stress rises.
This stage can bring mixed feelings. People are often proud of their progress and nervous about losing structure at the same time. That is normal.
If you're helping a loved one understand this handoff, it may help to read about what is transitional care. The concept is broader than addiction treatment, but the core idea fits here well. Recovery tends to go better when the move between levels of care is planned, supported, and matched to the person's actual risks.
Across all three phases, the timeline is adjusted to the person, not the calendar. For people who have relapsed before, extended care can be a sound treatment decision. It gives stabilization time to stick, therapy time to reach the underlying drivers of use, and discharge planning time to become something more than good intentions.
Why 90 Days or More Is the Gold Standard for Lasting Recovery
A family often asks this in a quiet voice during an intake call: “If they already went to rehab once, why would they need longer this time?”
It is a fair question. It can also carry shame. Many people hear “90 days or more” and assume it means the person is doing worse or failing treatment. In practice, a longer stay often means the care team is matching treatment to the pattern of the illness. If someone has a history of relapse, the goal is not to repeat the same short timeline and hope for a different result. The goal is to give recovery enough time to take root.
Longer care helps recovery hold under real-life pressure
A short stay can create safety and momentum. For some people, that is the right starting point. But addiction recovery is less like treating a sprained ankle and more like rebuilding strength after a serious injury. Early improvement matters, but it does not always predict what happens after discharge, when stress, conflict, boredom, grief, or old social contacts return.
That is one reason treatment programs often view 90 days as a strong benchmark for better outcomes. The National Institute on Drug Abuse's treatment overview notes that people with substance use disorders need enough time in treatment for the brain and behavior changes involved in addiction to begin improving. Recovery usually gets stronger with continued engagement, not a quick exit.
For someone who has relapsed before, more time can be a clinical strategy, not a punishment. A relapse history may signal that the first layer of treatment helped with stopping use, but did not give enough time to work through triggers, mental health symptoms, relationship patterns, or the return to daily life. Extending care gives those issues room to be addressed before the person is carrying them alone.
Ninety days is often a beginning, not a fixed finish line
Families sometimes hear “90 days” as if it were a magic number. It is better to picture it as a minimum stretch of time that often allows treatment to do its full job.
In the first weeks, people are often still physically and emotionally unsettled. After that, therapy can go deeper. Skills can be practiced repeatedly. Medications can be adjusted and monitored. Family work can start to shift old patterns. By the time a person reaches the later part of a longer program, clinicians have a clearer view of what support will still be needed.
That extra time matters even more for people with co-occurring depression, anxiety, trauma, or repeated return-to-use episodes. Their treatment plan may need more than one setting over time, including residential care, outpatient therapy, medication support, sober living, or convenient online treatment options. The longer timeline is not about keeping someone in rehab for its own sake. It is about building a plan that can keep working after formal treatment ends.
Extended treatment can be the more practical choice
Leaving too soon can create a false sense of readiness. A person may feel better inside a structured setting and still be unprepared for the pace and pressure of ordinary life. More time in care gives them more chances to practice honesty, ask for help sooner, repair routines, and respond to setbacks before a setback becomes a full relapse.
That is why longer treatment is often the more realistic option for lasting recovery, especially after prior attempts have not held. In addiction care, repeating a short stay is not always the most efficient path. Sometimes the wiser path is a longer one, because it gives the person a better chance to heal once and build on it.
How to Find the Right Level of Care at Addiction Resource Center

If you're trying to sort this out for yourself or someone you love, the next step isn't choosing a number. It's getting a professional assessment that looks at substance use, withdrawal risk, mental health, relapse history, home environment, and what kind of support is realistic.
What your first conversation should help clarify
A good intake call should answer practical questions without pressure. You should leave that call knowing whether detox is needed, whether residential care makes sense, and whether outpatient options could work safely.
For people who need flexibility because of work, family responsibilities, transportation, or distance, it can also help to understand convenient online treatment options. Telehealth isn't right for every stage of care, but for some people it makes ongoing treatment much more reachable.
Addiction Resource Center LLC in Yuba City offers a full continuum built for these decisions. That includes medically supervised detox with medication-assisted treatment, residential rehabilitation through its partner facility Ona Treatment Center in Browns Valley, and an Intensive Outpatient Program available in person and through telehealth.
What to ask before you commit
Ask direct questions. They matter.
- Which level of care do you recommend first, and why?
- If I've relapsed before, how would you adjust the timeline?
- What happens after detox or residential treatment ends?
- Do you help with insurance verification, including TRICARE?
- Can family members call for guidance before admission?
At Addiction Resource Center, care is delivered by a multidisciplinary team that includes a medical doctor, registered nurse, licensed counselors, an LMFT, and recovery mentors. Adults 18+ can get confidential guidance, individualized treatment planning, and support that stays grounded in real life rather than one-size-fits-all promises.
If you're asking how long does rehab take, the most honest answer is this: long enough to give recovery a real chance. Addiction Resource Center LLC helps adults and families in Northern California find the right starting point, whether that means detox, residential treatment through its partner facility, or in-person or telehealth IOP. The team offers compassionate, confidential support, accepts most major insurance plans including TRICARE, and can help you understand what level of care fits your situation. You can call or text 530-625-7910 anytime for a free, private conversation, or visit the center at 1002 Live Oak Blvd., Suite A, Yuba City, CA to take the next step.