You open the bathroom cabinet to put away a prescription bottle after your parent's surgery. The label says one tablet every few hours as needed. But the bottle is emptier than it should be. When you ask, they say the pain has been worse than expected, and they just needed a little more relief. That …
You open the bathroom cabinet to put away a prescription bottle after your parent's surgery. The label says one tablet every few hours as needed. But the bottle is emptier than it should be. When you ask, they say the pain has been worse than expected, and they just needed a little more relief.
That answer might be true. It might also be incomplete.
Many families find themselves in this difficult situation. You don't want to overreact. You also don't want to ignore something that could become dangerous. The question usually isn't about blame. It's about knowing whether you're looking at a medication mistake, a pattern of misuse, something that fits older ideas of abuse, or a problem serious enough to justify a professional assessment.
If you're trying to make sense of abuse vs misuse, you're not alone. The terms sound similar, but they don't mean the same thing. Neither term tells the whole story by itself. What matters most is what the behavior looks like over time, what consequences are showing up, and whether the person can still control their use.
Table of Contents
- Is It Abuse or Misuse When Do You Worry
- Defining the Terms Substance Misuse and Abuse
- A Detailed Comparison of Abuse vs Misuse
- Common Examples of Misuse and Abuse
- From Misuse and Abuse to a Substance Use Disorder
- When and How to Seek Help for a Loved One
- Find Help and Answers at Addiction Resource Center
Is It Abuse or Misuse When Do You Worry
A family usually notices the pattern before the person using the substance does. It may start with small things. Pills run out early. Refills become urgent. Someone seems more irritable, sleepy, or secretive. They insist they're only trying to manage pain, stress, or sleep.
That's why this question feels so hard. The behavior may not look dramatic at first. A person may still be going to work, showing up for family dinners, and saying all the right things. But you can still sense that something isn't right.
The first question isn't who is at fault
In counseling, I tell families to stop asking, “Is this bad enough to count?” and start asking, “Is this changing the person's safety, judgment, or daily life?” That shift helps. It moves the conversation away from labels and toward risk.
A person can misuse a medication without setting out to get high. They can also move from a medical reason into a dangerous pattern faster than the family expects. What matters is not just the original reason for taking it. What matters is whether the use is becoming harder to control.
Practical rule: If you're seeing repeated problems, secrecy, or escalating use, it's reasonable to take it seriously even if the person says the reason is still medical.
What families usually miss
Many people think misuse is minor and abuse is severe. Real life isn't that neat. These terms describe patterns, but people don't always stay in one category. Someone can begin by taking more than prescribed because they're hurting, then start relying on the drug to cope with stress, sleep, or emotions.
If your gut is telling you something has changed, pay attention. You don't need to prove a diagnosis before reaching out for guidance. You only need enough concern to say, “This may need a closer look.”
Defining the Terms Substance Misuse and Abuse
The easiest way to understand misuse is this. A person is using a substance in the wrong way, even if the reason still sounds medical or practical. They may take more than directed, take it more often, use it longer than instructed, or use a medication that wasn't prescribed to them.
The clearest public health definition comes from SAMHSA's National Survey on Drug Use and Health. It treats misuse as use without one's own prescription or use in greater amounts, more often, or longer than told to take a drug, even when the goal is pain relief. In that same reporting framework, 7.6 million people age 12 and older misused prescription opioids in the past year in 2024, and 45.2% of those cases involved hydrocodone products, according to the 2024 NSDUH national report.
What misuse usually looks like
Misuse often sounds like this:
- “I took an extra one because the pain was bad.”
- “I borrowed my sister's pills because I couldn't sleep.”
- “I kept taking the medication after the prescription should have ended.”
The person may still believe they're solving a real problem. That doesn't make it safe.
What people often mean by abuse
Older everyday language often uses abuse to mean using a substance for non-medical reasons, especially to feel intoxicated, escape feelings, or change mood. Families often use the word when the behavior looks more deliberate, more repeated, or more harmful.
That said, this word can create confusion. Some people hear “abuse” and think it only applies if someone is using street drugs or intentionally trying to get high every time. Others hear it as a moral judgment instead of a description of harmful behavior.
The most useful distinction is often intent plus pattern. Misuse is inappropriate use that may begin with a therapeutic or practical reason. Abuse is commonly understood as use despite harm, often with a non-therapeutic goal.
Why the distinction matters
When you understand the terms, you can ask better questions:
- Is the substance prescribed to them?
- Are they following directions?
- Has the reason for using it changed?
- Are problems appearing at home, work, or in health?
Those questions matter more than winning an argument over vocabulary. They help you decide whether you're dealing with a one-time lapse, a repeating pattern, or a sign that professional help is needed.
A Detailed Comparison of Abuse vs Misuse
The difference between abuse vs misuse becomes clearer when you compare them side by side. Families often get hung up on a single incident, but a better approach is to look at intent, pattern, and consequences together.
Comparison of Substance Misuse vs Abuse
| Criterion | Substance Misuse | Substance Abuse |
|---|---|---|
| Intent | Usually starts with a therapeutic, practical, or self-directed reason | Often involves using the substance for intoxication, escape, or other non-therapeutic effects |
| Prescription status | May involve using one's own prescription incorrectly or using someone else's medication | May involve prescribed or non-prescribed substances used for desired psychoactive effects |
| Pattern | Can be occasional or repeated | More often persistent, escalating, or harder to stop |
| How the person explains it | “I needed relief,” “I needed sleep,” “I had to get through the day” | “I wanted to relax,” “I wanted to feel different,” or explanations that hide the real purpose |
| Risk | Still dangerous because dosage, timing, and medical oversight are off | Dangerous because the use itself is tied to harm and loss of control |
| Family warning sign | Running out early, borrowing medication, taking more than directed | Secrecy, craving, repeated harmful consequences, using despite obvious problems |
Sometimes readers find this kind of distinction helpful in other difficult topics too. If you've ever had trouble separating two terms that sound similar but lead to very different responses, this guide from WeUnite can also clarify bullying and harassment in a similarly practical way.
Why professionals separate the terms
In safety monitoring, these terms aren't treated as interchangeable. The FDA pharmacovigilance framework separates them on purpose. It defines misuse as “any intentional therapeutic use of a drug product in an inappropriate way,” while abuse is tracked separately as an Abuse Event Indicator within a broader system that also watches diversion, tampering, withdrawal, and overdose, as described in this FDA-focused pharmacovigilance review.
That matters because it reflects what families see in real life. Two people may take the same medication incorrectly, but the context is different. One person may be trying to treat pain badly. Another may be seeking intoxication. The safety response, clinical questions, and risk level can differ.
What to pay attention to at home
Don't focus only on what the person says their intent is. Watch what the behavior is doing.
- Escalation matters: Are they taking more over time?
- Preoccupation matters: Do they seem unusually focused on refills, dosing, or access?
- Impact matters: Are relationships, mood, responsibilities, or health being affected?
A single episode of misuse deserves attention. A repeated pattern with growing fallout deserves assessment.
Common Examples of Misuse and Abuse
Real examples make these terms easier to spot. Most families don't walk around using clinical language. They notice situations.
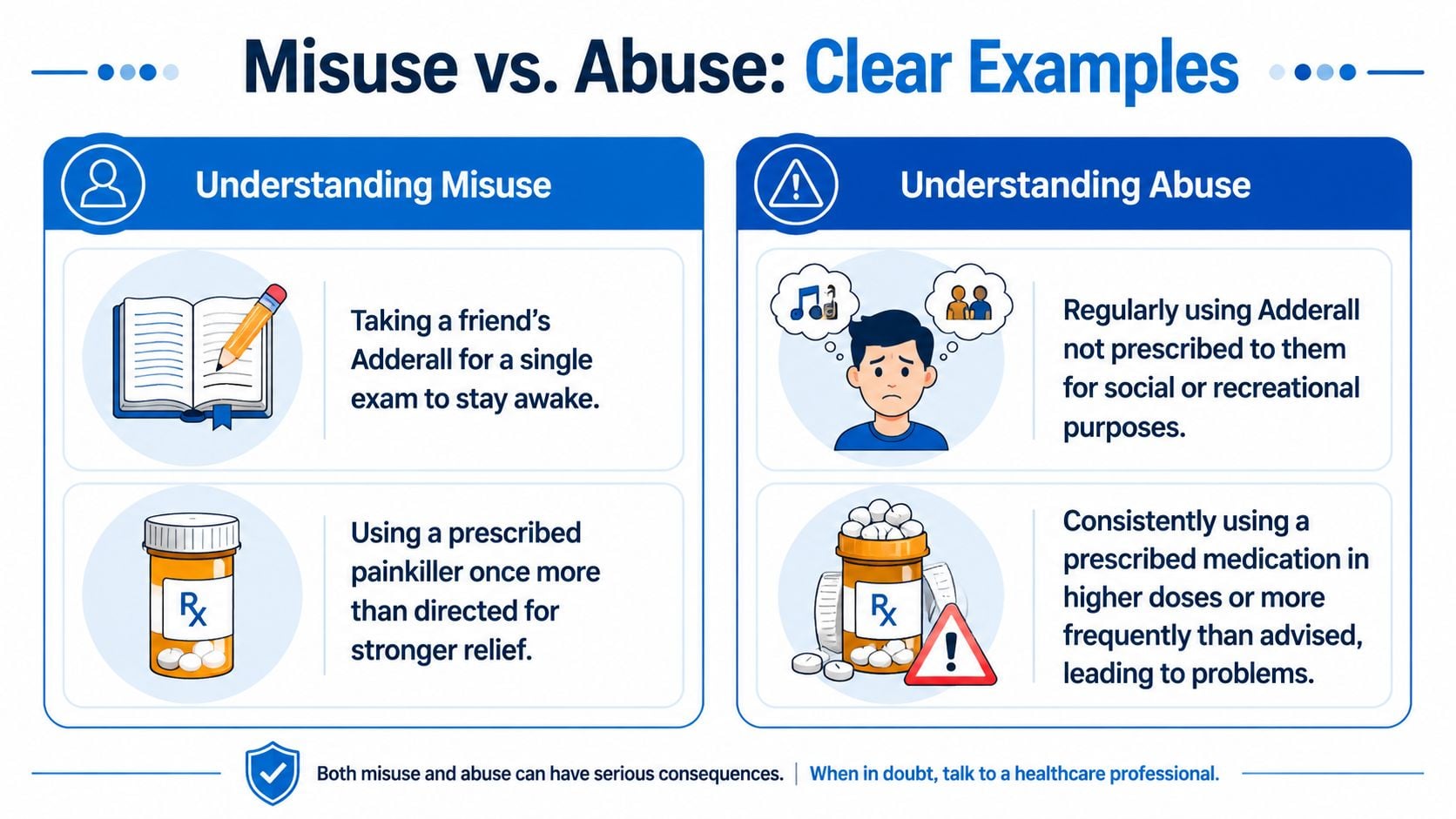
Examples that fit misuse
A college student takes a friend's Adderall the night before one exam because they want to stay awake and focus. They tell themselves it's just this once, and they're using it to study, not to party.
A man recovering from dental surgery takes more of his prescribed pain medication than directed because he says the pain is stronger than expected. He doesn't call the prescriber first. He just increases the dose on his own.
A woman with insomnia takes one more sleeping pill than instructed after a hard week because she feels desperate for rest. She still sees it as a sleep solution, not a drug problem.
Examples that fit abuse
A person regularly uses someone else's stimulant medication at parties because they like the way it makes them feel. The goal isn't treatment. The goal is the effect.
Another person keeps seeking opioid prescriptions from different sources and uses the medication in a way that clearly goes beyond medical care. They may still talk about pain, but the pattern centers on continued access and continued use despite problems.
Someone drinks specifically to numb grief, anger, or anxiety night after night, even as relationships and responsibilities start slipping. The substance has become a coping tool that creates more damage than relief.
Where the gray area appears
The gray area is where many serious problems begin. Misuse can drift into something more entrenched. A person may start with a real symptom, then begin to rely on the substance for stress, emotions, or daily functioning.
One reason this matters is that misuse doesn't always stay small. A recent national summary reported 13.8 million people misused prescription drugs in a year, and 55.3% of people who misuse prescriptions were classified as definitively addicted, according to these prescription drug misuse statistics.
If you're watching a loved one cross from occasional rule-breaking into increasing dependence, you're not being dramatic by getting concerned. You're noticing the point where risk grows.
The key question isn't whether an example fits perfectly into one box. The key question is whether the use is becoming more frequent, more harmful, and less controllable.
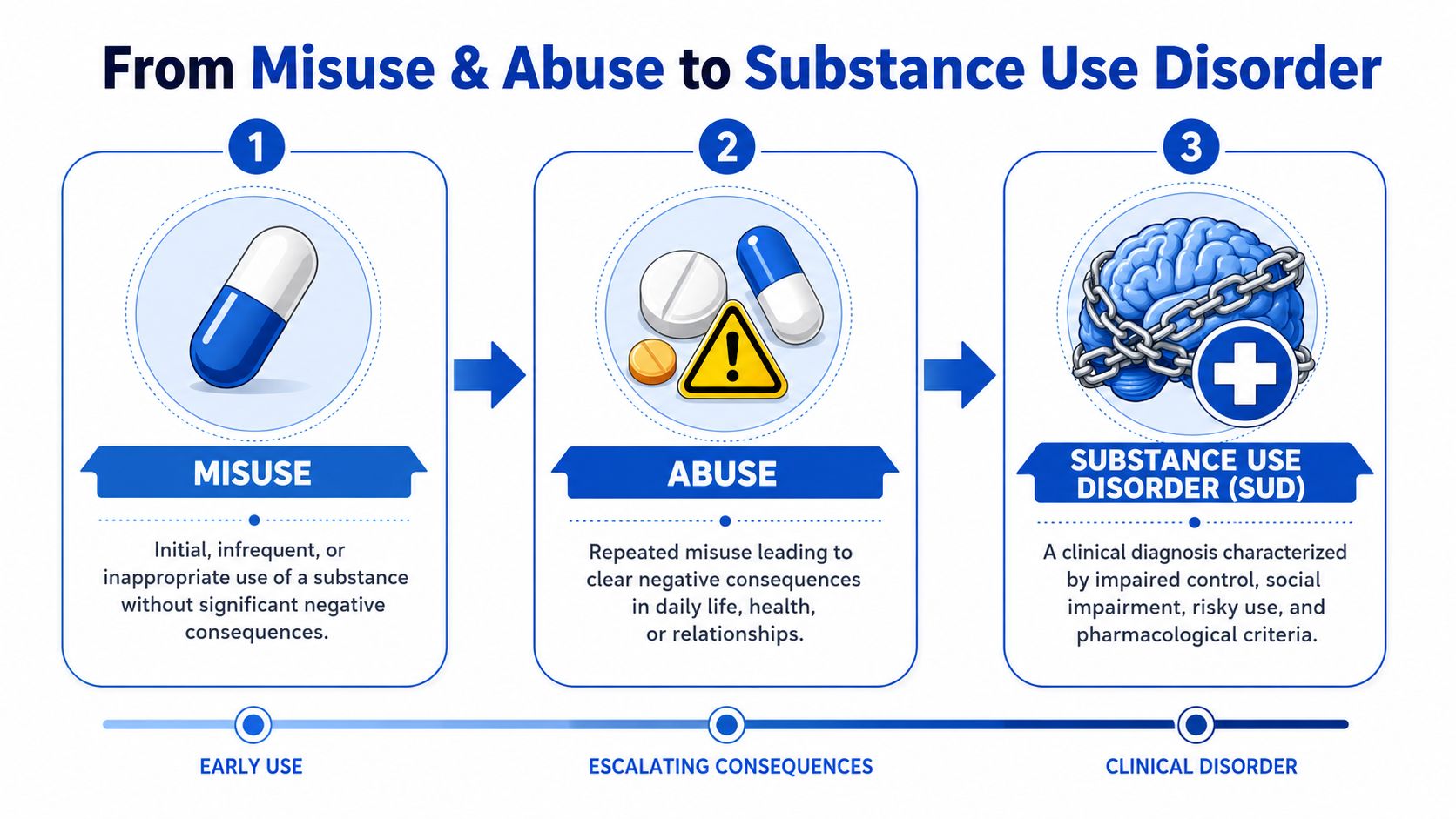
From Misuse and Abuse to a Substance Use Disorder
Terms like misuse and abuse describe behavior. Substance use disorder describes a clinical condition. That distinction matters because families often see the behavior first and don't realize it may point to something diagnosable and treatable.
Why the language has changed
Many clinicians now prefer broader, less stigmatizing language. Rather than centering the older word “abuse,” they talk about substance use, substance misuse, and substance use disorder. That helps separate a behavior from a person's identity.
A review in NIH-linked literature notes that many authoritative sources favor these broader terms, while the APA has defined substance abuse as continued use despite harm. That same literature also points out that older terminology can blur intent and severity, which is one reason clinical language has shifted, as discussed in this overview of substance use terminology and concepts.
When behavior becomes a clinical condition
A disorder is not just “using badly.” It's a pattern where the person keeps using despite consequences, struggles to cut down, or shows impaired control around the substance. By the time families are asking whether it's abuse vs misuse, they may already be seeing clues that the issue has moved beyond a one-off incident.
Watch for clusters of change such as:
- Control problems: They say they'll cut back and can't.
- Life disruption: Work, parenting, school, or relationships start suffering.
- Risky persistence: They continue even after obvious harm.
A useful question is not “Would a professional judge this?” It's “Has this become bigger than willpower, promises, or home rules can manage?”
That's the moment when assessment matters. You don't have to wait until everything falls apart. If the person's use is becoming more central to daily life, causing repeated consequences, or taking over how they cope, it may be time to treat the behavior as a health issue rather than a character issue.
When and How to Seek Help for a Loved One
Your sister says she is fine. Then you notice she has run out of pills early again, missed a family event, and snapped at you when you asked about it. Families often get stuck here. They are not only asking, "Is this misuse or abuse?" They are asking a more practical question. "At what point do we stop debating words and get a professional involved?"
A useful way to look at it is this: a single poor decision can happen in many homes, but a repeating pattern needs attention. If substance use keeps showing up as the reason for conflict, missed responsibilities, risky behavior, or personality changes, it is time to consider an assessment. You do not have to wait for a disaster before asking for help.
This visual summary can help organize what to look for first.
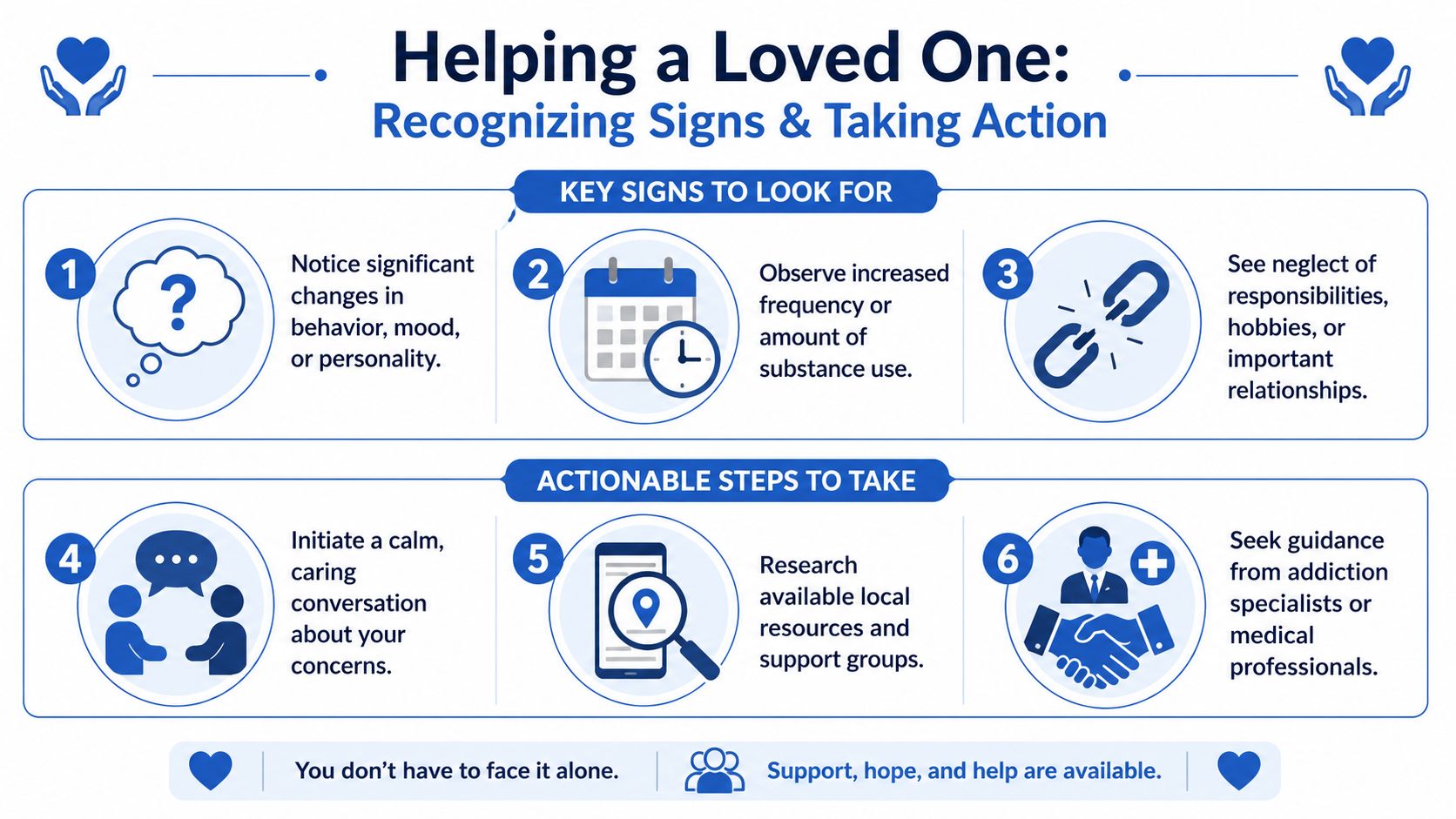
Signs that it is time for an assessment
Families sometimes worry they need proof before they reach out. They do not. An assessment is not a verdict. It works more like a medical checkup for a confusing pattern. The goal is to find out what is happening, how serious it is, and what kind of help fits.
A professional evaluation makes sense when you are seeing concerns like these:
Use is becoming more frequent or harder to predict
The person is using more often, taking higher amounts, or seeming preoccupied with getting or using the substance.Daily life is shrinking around the substance
Work, school, parenting, sleep, hygiene, or relationships are starting to slip.Honest conversations keep stalling out
You bring up specific concerns and get denial, anger, blame, or repeated promises that do not lead to change.Safety questions keep coming up
You are worried about driving, falls, mixing substances, withdrawal, overdose, or children being affected by the situation.
National treatment reports continue to show a large gap between people who need help and people who receive it, as described in this summary of national treatment need and access. That gap is one reason families benefit from acting early, before the pattern becomes harder to interrupt.
How to start the conversation
Timing matters. Bring it up when the person is sober, as calm as possible, and not rushing out the door. A hard conversation usually goes better when it feels like concern, not prosecution.
Try simple, concrete language:
- “I'm concerned because I've seen you take more than prescribed more than once.”
- “I care about you, and I want us to get a clearer picture of what's going on.”
- “Would you be open to talking with a professional who can assess this?”
Keep the focus on what you have observed. That means dates, behaviors, missed events, changes in mood, or safety problems. It helps to avoid labels, old arguments, and guesses about why they are using. Families often get farther when they speak the way a doctor would. Calm, specific, and focused on patterns.
Sometimes the picture is more complicated because substance use and mental health symptoms feed each other. If your loved one seems to be dealing with both alcohol use and depression, it may help to read about integrated care for depression and alcohol, since coordinated treatment is often more effective than addressing only one issue.
A brief video can also help families frame the conversation and the next steps.
What to do next
If your loved one agrees to get help, start with an assessment by a medical provider, addiction counselor, or treatment program. That first appointment helps answer practical questions. Is this occasional misuse, a developing substance problem, withdrawal risk, or a sign that a higher level of care is needed?
If they refuse, you still have options. You can get guidance for yourself on boundaries, safety planning, and how to respond in a consistent way. Family support does not depend on the other person being ready today.
Treatment options may include outpatient counseling, medication-assisted treatment, medically supervised detox, or a higher level of care based on the substance involved, the risk of withdrawal, and how much the problem is affecting daily life. In Northern California, Addiction Resource Center LLC is one option that offers medically supervised detox with medication-assisted treatment, outpatient support, and telehealth services for adults seeking substance use care.
The main goal is to get a clear assessment and act on it. Once a pattern begins to affect safety, health, or daily functioning, professional help becomes the next sensible step, not an overreaction.
Find Help and Answers at Addiction Resource Center
If your family has reached the point where concern keeps repeating, a direct next step can make things feel more manageable. Sometimes the hardest part is not deciding whether you're worried. It's figuring out who to call first.

A treatment center can help sort out what you're seeing. That may include whether the issue looks like prescription misuse, a broader substance use problem, withdrawal risk, or a need for coordinated mental health support. Families don't have to solve that alone.
For people in Yuba City and nearby Northern California communities, the available services described by the provider include medically supervised detox with medication-assisted treatment, residential rehabilitation through a partner facility, and an Intensive Outpatient Program offered in person and through telehealth. The care model also includes licensed counselors, medical staff, and recovery support, along with aftercare planning.
Practical details matter too. The location is 1002 Live Oak Blvd., Suite A, Yuba City, CA, and the provider lists a 24/7 phone/text line at 530-625-7910. It also states that it accepts most major insurance plans and welcomes TRICARE beneficiaries.
If you're unsure whether your loved one needs treatment, that uncertainty itself is often a reason to ask for an assessment. You don't have to wait until the situation becomes unmistakable. Early questions are easier to address than late crises.
If you need a clear next step, Addiction Resource Center LLC offers a practical place to start. You can reach out to ask about an assessment, treatment options, insurance, detox, outpatient care, or how to support a loved one who may be struggling.