
Learn dual diagnosis treatment basics and how integrated care addresses co-occurring mental health and substance use disorders effectively.

Having both a mental health disorder and a substance use disorder at the same time is more common than most people realize. Yet many people struggling with this combination never get proper treatment because the conditions mask each other.
At Addiction Resource Center, we’ve seen firsthand how dual diagnosis treatment basics matter-when you treat only addiction or only depression, the other condition often sabotages recovery. This guide walks you through what integrated care looks like and how it actually works.
Understanding Co-Occurring Disorders
What Defines Dual Diagnosis
Co-occurring mental health and substance use disorders means a person has both conditions at the same time, and they interact in ways that complicate treatment. This isn’t two separate problems that happen to exist in one person-the conditions feed each other. Someone with depression might drink to escape symptoms, which worsens depression over time. Someone with anxiety might use stimulants to feel in control, which intensifies panic attacks. The substances alter brain chemistry in ways that make mental health symptoms harder to treat, and untreated mental illness drives substance use escalation.
According to SAMHSA’s 2024 National Survey on Drug Use and Health, approximately 21.2 million adults in the United States had co-occurring mental illness and substance use disorder. That’s not a small subset-it’s a massive portion of people struggling with addiction. The most common mental disorders in dual diagnosis cases include anxiety disorders, mood disorders like major depression, PTSD, bipolar disorder, and schizophrenia. Substances involved range from alcohol and opioids to stimulants, marijuana, and prescription drugs misused outside their intended use.
Why Treatment Systems Miss Dual Diagnosis
Treatment systems are built to catch one problem at a time. Mental health clinics focus on depression or anxiety and may not screen for alcohol use. Addiction treatment programs concentrate on substance use and might overlook the anxiety that drives the drinking. When a person shows up to treatment for depression and admits to drinking, clinicians sometimes assume the alcohol use will resolve once depression improves-it rarely does.
SAMHSA’s no wrong door policy exists specifically because this gap is so dangerous. It means screening for substance use should happen routinely in mental health settings and mental health screening should be standard in substance use treatment. Without this dual screening approach, people fall through cracks. A person with undiagnosed PTSD and alcohol use disorder receives treatment only for the drinking, relapses when trauma triggers emerge, then gets labeled treatment-resistant. Another person with bipolar disorder receives psychiatric care but no addiction support, cycles through hospitalizations driven partly by substance use, and never achieves stability.
The Real Cost of Missed Dual Diagnosis
The statistics show this matters: people with co-occurring mental health and substance use disorders are more likely to be hospitalized than those with only one disorder. Treatment non-adherence runs higher. Relapse rates climb. Recovery capital-the resources someone has like employment, stable housing, and social support-tends to be lower in dual diagnosis populations because the conditions compound each other’s damage.
This fragmentation in care creates a cascade of problems. A person bounces between mental health and addiction providers, each treating their piece of the puzzle while the whole picture remains invisible. Medications prescribed by one doctor interact with substances the other doctor doesn’t know about. Progress stalls. Frustration builds. The person concludes they’re untreatable when the real problem is that nobody’s treating both conditions together. Understanding how integrated care changes this dynamic requires looking at what actually works when treatment addresses both disorders simultaneously.
Why Single-Disorder Treatment Fails With Dual Diagnosis
The Predictable Collapse of Fragmented Care
A person with depression and alcohol use disorder completes a 28-day addiction program, leaves sober, then crashes within weeks because untreated depression makes sobriety unbearable. Another person receives antidepressants and therapy for anxiety but no addiction support, continues using stimulants to manage panic, and finds the drugs counteract their medication. The two disorders don’t exist in separate compartments-they reinforce each other constantly. When treatment addresses only one, the other sabotages recovery from the start.
Research from SAMHSA shows that people with co-occurring disorders who receive fragmented care experience higher hospitalization rates than those with only one disorder. They also show worse treatment adherence and faster relapse cycles. The problem isn’t that people lack motivation or commitment. The problem is that isolated treatment ignores the biological and behavioral reality: substance use changes brain chemistry in ways that worsen psychiatric symptoms, and untreated mental illness drives continued substance use as a coping mechanism.
How Integrated Treatment Reverses the Cycle
Integrated treatment flips this dynamic by treating both conditions simultaneously through the same provider or coordinated team. A therapist trained in both addiction and mental health works with you on depression and drinking in the same sessions, addressing how they feed each other rather than treating them as unrelated issues.
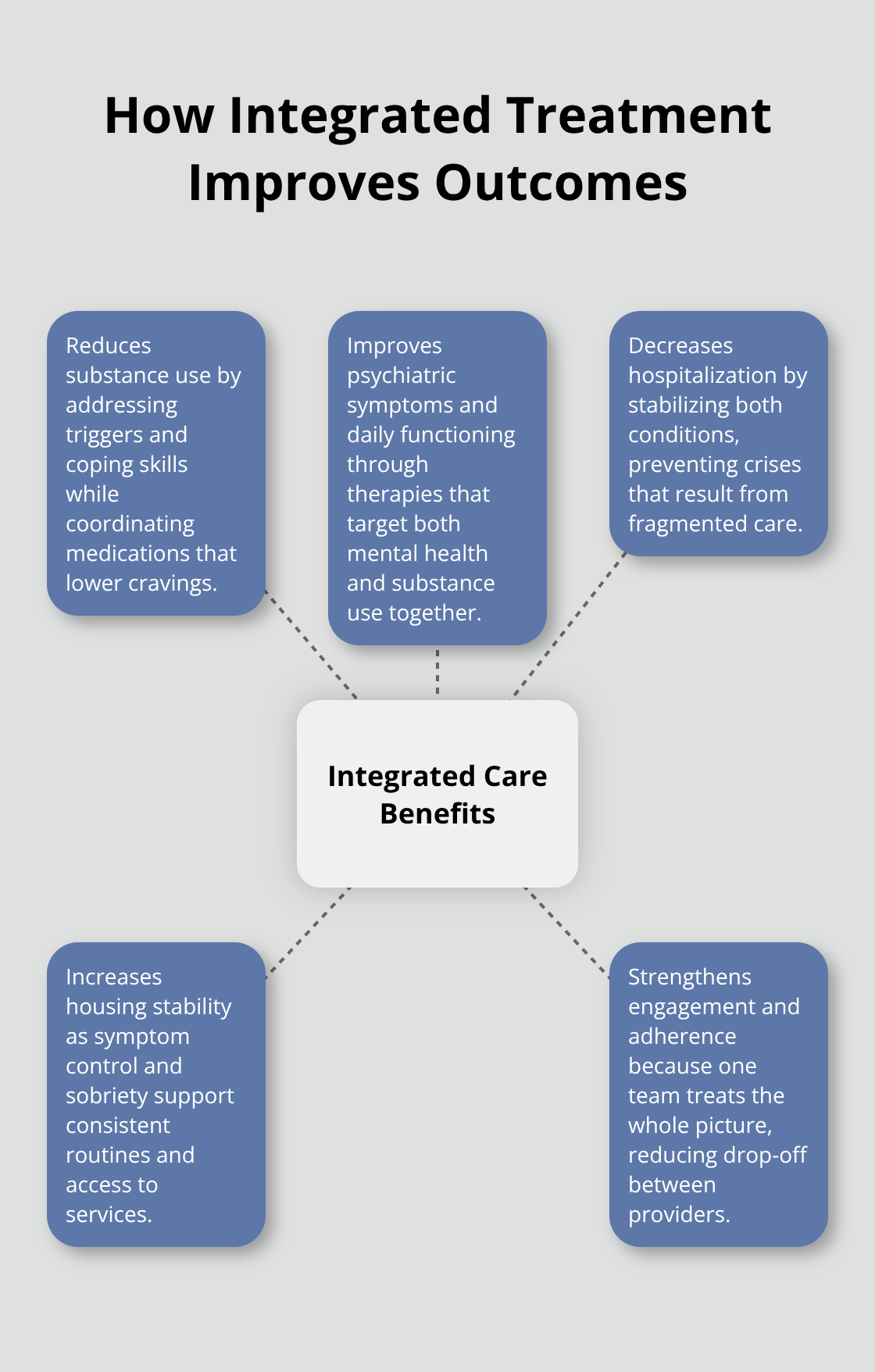
Integrated care reduces substance use more effectively than coordinated or sequential approaches, producing reduced substance use, improvement in psychiatric symptoms and functioning, decreased hospitalization, and increased housing stability.
One Norwegian study comparing integrated treatment to standard mental health care found that integrated programs significantly increased motivation for sustained recovery after 12 months, even when substance use reductions were similar between groups. That motivation shift matters because it predicts long-term outcomes.
Coordination That Actually Works
Integrated programs coordinate medications so an antidepressant doesn’t conflict with substance use patterns, and they address housing, employment, and social support as part of treatment rather than afterthoughts. When a therapist understands both your depression and your addiction, they catch the real triggers-the anxiety spike that leads to drinking, the shame from substance use that deepens depression-and treat the cycle itself rather than isolated symptoms.
This coordinated approach means your treatment plan reflects your actual life, not a theoretical version of it. Your provider knows what you’re taking, what you’re using, and what situations push you toward relapse. They adjust medications and therapy based on how both conditions respond together. This level of coordination is what separates treatment that sticks from treatment that collapses.
Understanding how integrated care actually operates in practice requires looking at the specific evidence-based methods that make this approach work.
Evidence-Based Treatment Methods for Dual Diagnosis
Medication-Assisted Treatment That Addresses Both Conditions
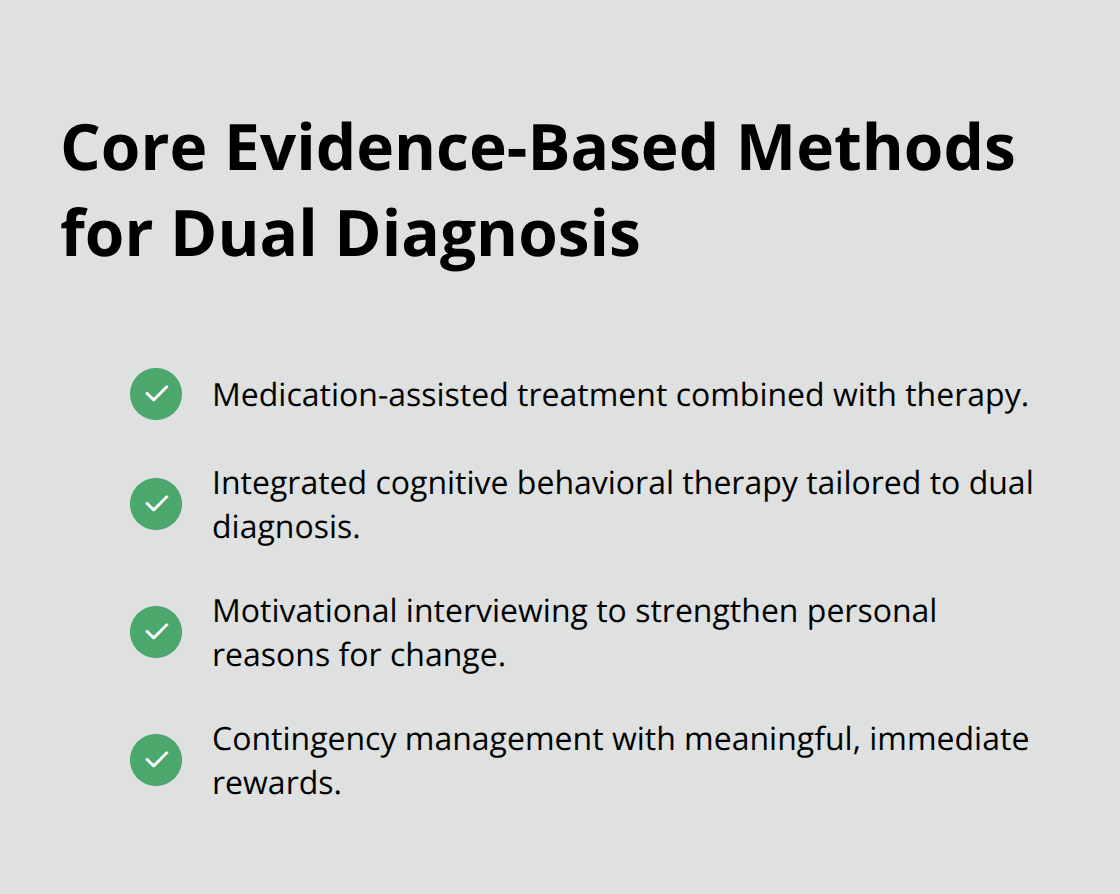
Medication-assisted treatment combined with therapy addresses the biological reality that dual diagnosis requires both pharmaceutical and behavioral intervention. When someone has depression and alcohol use disorder, antidepressants alone will not stop drinking, and addiction treatment without psychiatric medication leaves depression untouched. The research is clear: medications like naltrexone or acamprosate reduce cravings for alcohol while antidepressants stabilize mood, but only when a therapist trained in both addiction and mental health monitors how they interact. A study published in SAMHSA’s treatment improvement protocols found that people receiving coordinated medication management across both conditions showed better treatment adherence than those receiving either approach in isolation.
The key is that your prescriber must know about all substances you use and all psychiatric symptoms you experience, because stimulant medications can worsen anxiety in someone with PTSD, and certain antidepressants can interact with opioids in dangerous ways. Your medication plan reflects your actual situation, not a theoretical version of it. Providers who coordinate across both conditions prevent these conflicts before they sabotage your recovery.
Cognitive Behavioral Therapy Adapted for Dual Diagnosis
Cognitive behavioral therapy specifically adapted for dual diagnosis works differently than standard CBT because it targets the exact cycle linking your mental health and substance use. Instead of treating depression separately from drinking, integrated CBT identifies how negative thoughts trigger substance use and how substance use reinforces negative thoughts, then breaks that pattern. Research shows that integrated CBT approaches reduce both psychiatric symptoms and substance use more effectively than treating either condition alone, with particular strength in reducing PTSD symptoms when combined with trauma-focused modules like Seeking Safety.
The therapy sessions focus on concrete situations from your life: the specific moment when anxiety spikes and you reach for alcohol, the shame after using that deepens depression, the relationships damaged by both conditions. Your therapist teaches you to recognize these triggers and practice alternative responses before they happen, not in theory but through role-play and homework assignments tied to your actual environment. This targeted approach addresses the real mechanisms that keep dual diagnosis cycling.
Motivational Interviewing and Contingency Management
Motivational interviewing paired with contingency management creates accountability while respecting your autonomy in recovery. Motivational interviewing addresses the reality that people with dual diagnosis often feel ambivalent about change because untreated mental illness makes motivation itself difficult.
A therapist using this approach does not lecture or shame but instead helps you explore why you want to recover and what barriers exist, then builds on your own reasons for change rather than imposing external ones.
Contingency management adds structure by providing concrete rewards for meeting treatment goals like attending sessions, staying abstinent, or taking medications as prescribed. Studies show this combination significantly increases motivation for sustained recovery, and that motivation shift predicts whether people maintain gains after treatment ends. The rewards do not need to be large, just meaningful and immediate, because the brain in dual diagnosis requires reinforcement that is tangible and timely to overcome the dopamine dysregulation that both mental illness and substance use create.
Getting Started With Dual Diagnosis Treatment
Finding the right program starts with screening that catches both conditions. SAMHSA’s National Helpline at 1-800-662-4357 and FindTreatment.gov connect you to integrated programs in your area, and when you call, ask whether providers screen for both mental health and substance use, whether the same therapist or team addresses both conditions, and whether they offer medication management alongside therapy. Programs using SBIRT (Screening, Brief Intervention, and Referral to Treatment) have proven track records of identifying dual diagnosis early and moving people into appropriate care quickly. Your first weeks focus on medical safety, accurate diagnosis of both conditions, and building trust with your treatment team through comprehensive assessment that measures both psychiatric symptoms and substance use severity.
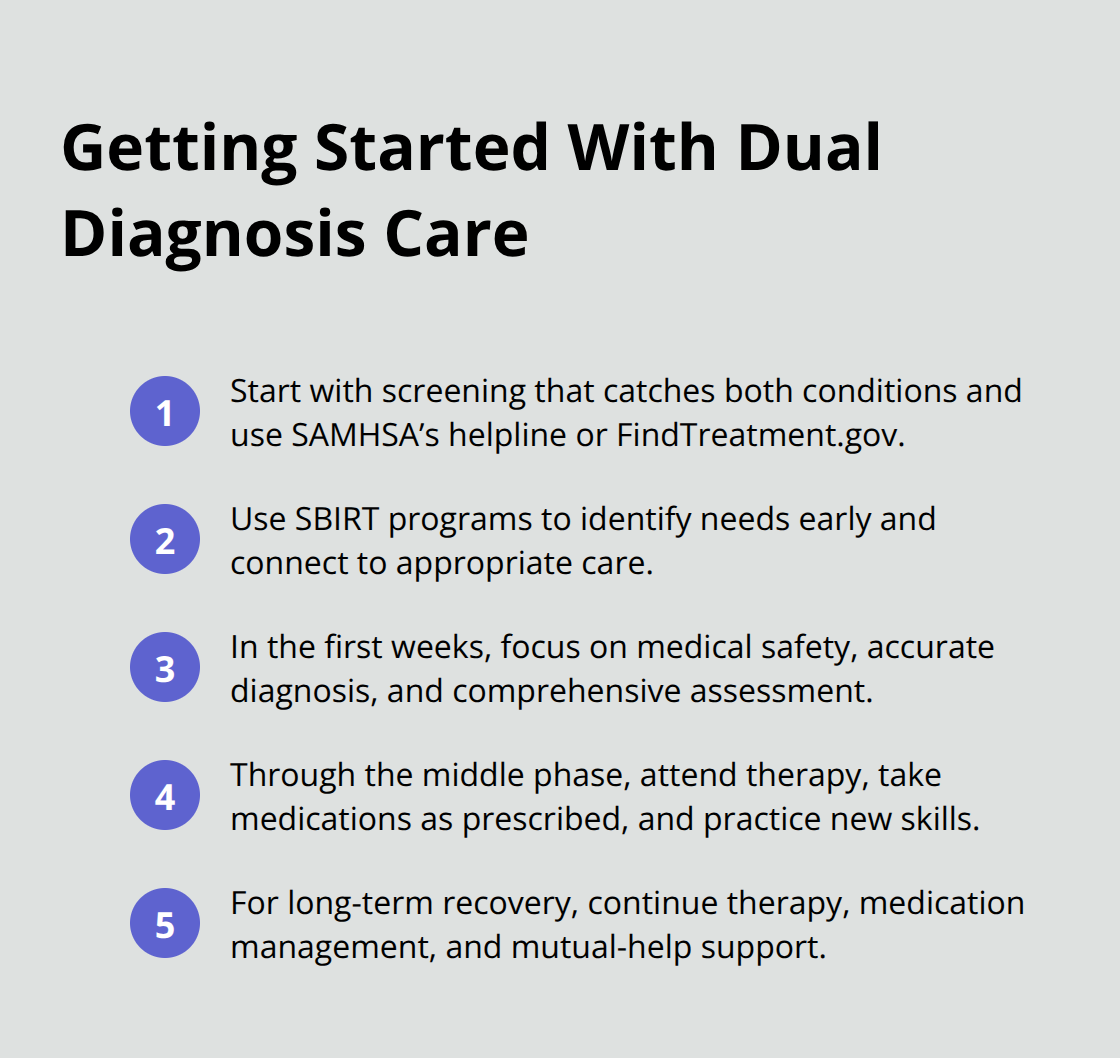
The middle phase of treatment is where dual diagnosis treatment basics become your daily practice. You attend therapy sessions, take medications as prescribed, and practice the skills your therapist teaches you-motivational interviewing helps you stay committed when ambivalence emerges, contingency management provides concrete rewards for meeting goals, and cognitive behavioral therapy adapted for dual diagnosis helps you recognize the specific triggers linking your mental health and substance use. This phase typically lasts weeks to months depending on your needs, and your provider adjusts medications and therapy based on how both conditions respond together.
Long-term recovery requires ongoing support after formal treatment ends, and people with dual diagnosis benefit from continued therapy, medication management, and mutual-help groups. We at Addiction Resource Center in Yuba City provide outpatient addiction treatment and mental health support designed to sustain recovery beyond initial treatment through personalized addiction therapy and substance abuse counseling tailored to your specific needs. Our compassionate approach recognizes that dual diagnosis recovery is not linear, and setbacks do not mean failure-what matters is returning to treatment quickly when needed and building a life where recovery becomes easier than relapse.



