If you're reading this late at night, searching how long does it take to recover, you're probably carrying more than one question. You may be wondering how long your son will need treatment, whether your spouse will ever feel like themselves again, or whether this is the start of a few hard months or a …

If you're reading this late at night, searching how long does it take to recover, you're probably carrying more than one question. You may be wondering how long your son will need treatment, whether your spouse will ever feel like themselves again, or whether this is the start of a few hard months or a much longer road.
Families usually ask for a number because they want relief. They want something they can circle on a calendar. The hard truth is that addiction recovery rarely works like that. The hopeful truth is that recovery does follow patterns, and when you understand those patterns, the process feels less mysterious and less frightening.
What helps most is replacing one big question with better ones. What happens in detox? How long do residential and outpatient care usually last? Why does alcohol recovery look different from opioid recovery? What changes when depression, trauma, or anxiety are part of the picture? Those are the questions that lead to realistic plans and better support.
Table of Contents
- Why There Is No Single Answer to How Long Recovery Takes
- The Stages of Recovery A Timeline Across Levels of Care
- How Different Substances Impact Your Recovery Timeline
- Personal Factors That Shape Your Recovery Journey
- Key Milestones What to Expect in Early and Long-Term Recovery
- How Loved Ones Can Support the Recovery Process
- Starting Your Journey Finding Treatment and Navigating Insurance
Why There Is No Single Answer to How Long Recovery Takes
A father once asked me, "Just tell me if this is a 30-day problem or a 5-year problem." That question holds a lot of pain. It also shows how recovery is often pictured, as if it has one start date, one treatment program, and one clean finish line.
Recovery is usually not one event. It's a series of stages. A person may move from withdrawal management, to therapy, to learning routines, to rebuilding trust, to handling stress without substances. Each stage asks the brain and body to do something different.
That matters because two people can both say, "I'm in recovery," while living very different realities. One may still be physically unstable and exhausted. Another may be sober for many months but just starting to work through trauma, grief, or shame. Both are recovering. They're in different phases.
Recovery has phases, not one finish line
When people ask how long does it take to recover, they often mean one of three things:
- How long until withdrawal eases: This is the shortest timeline, and it's only the beginning.
- How long until treatment is done: This depends on the level of care and whether the person needs detox, residential treatment, outpatient care, or all three.
- How long until life feels stable again: This is usually the longest timeline because it includes relationships, routines, emotional regulation, and relapse prevention.
Recovery gets easier to understand when you stop asking for one deadline and start looking at the next milestone.
A useful way to think about addiction is this. Detox clears the substance. Treatment teaches skills. Time and consistent support help those skills hold up in ordinary life. If a person leaves care too soon, they may be physically better but still emotionally unprepared for cravings, conflict, loneliness, boredom, or old habits.
Why the same diagnosis can still lead to different timelines
Two people with the same substance problem can recover at different speeds because their lives are different. One may have strong family support, stable housing, and no history of trauma. Another may be managing anxiety, legal stress, chronic pain, and a home environment where substances are still present.
Neither person is doing recovery wrong.
They're carrying different loads, and the timeline reflects that. The most helpful answer is not "it depends" in a vague way. It's that recovery follows a road map, but each person's road has different turns, obstacles, and support needs.
The Stages of Recovery A Timeline Across Levels of Care
Most families feel calmer once they can see the treatment path in order. Instead of one big blur called rehab, it helps to picture recovery as a continuum. Each level of care has a job.
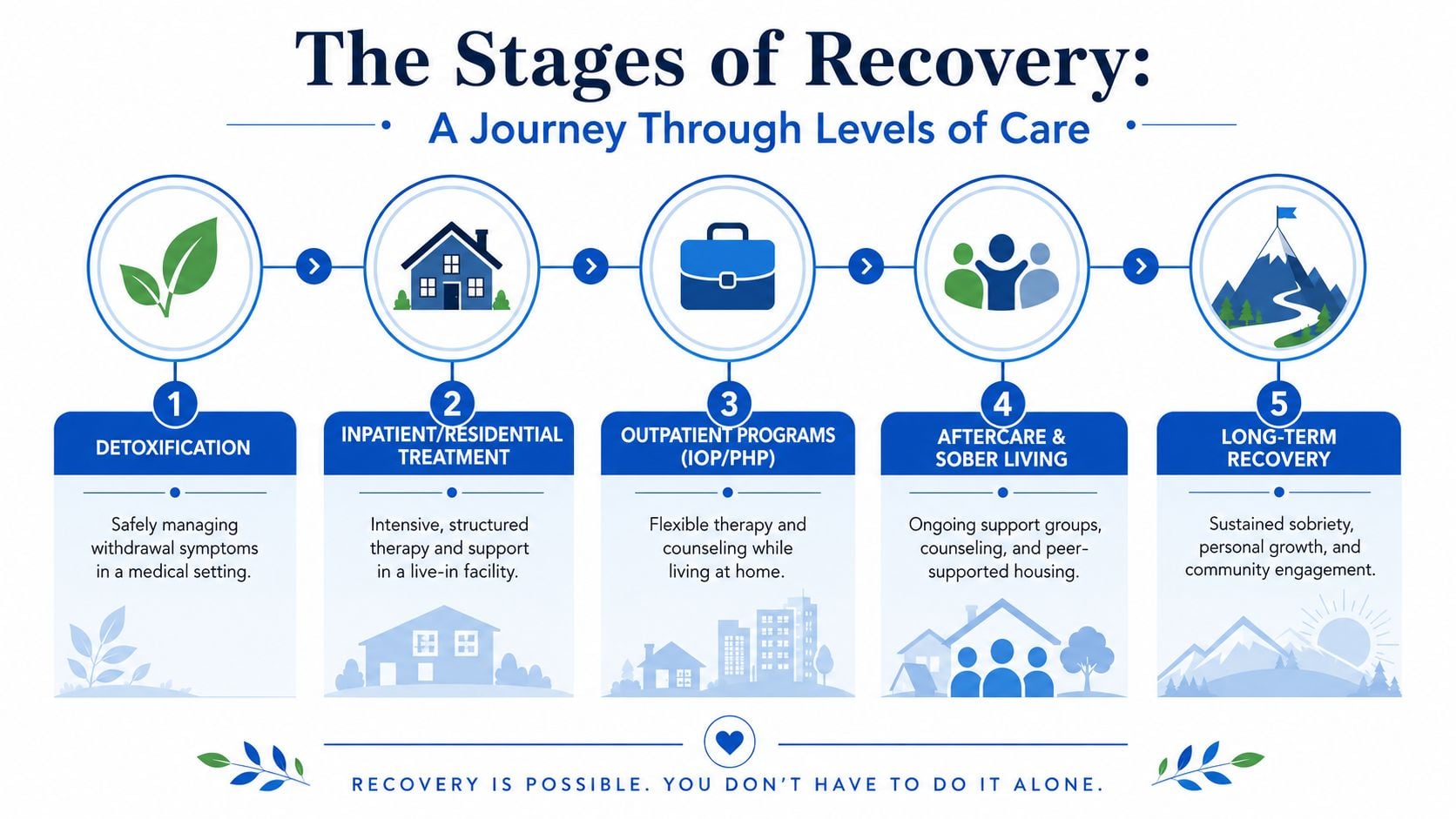
Detox is about safety and stabilization
Detox is the first phase when someone needs medical help to stop using safely. Families often focus on this stage because it's urgent. The person may be sick, frightened, restless, or at risk for dangerous withdrawal symptoms.
In plain language, detox is about getting the body through the first shock of stopping. It is not full recovery. It is the part where medical staff monitor symptoms, adjust medications when needed, support hydration, sleep, and nutrition, and help the person become stable enough for therapy to work.
A typical detox day may include:
- Medical check-ins: Staff monitor withdrawal symptoms, sleep, blood pressure, and comfort.
- Medication support: Some substances call for specific medications and careful timing.
- Short counseling contacts: Early conversations focus on immediate needs and readiness for the next step.
- Rest and basic care: People often need quiet, food, fluids, and reassurance before they can do deeper emotional work.
Residential care builds structure
Residential treatment comes next for people who need a live-in setting with daily support. Within this setting, recovery starts to get more organized. The schedule itself becomes part of treatment. People wake up at regular times, attend therapy, eat meals on time, and begin practicing a different kind of life.
The goal here is broader than stopping substance use. Residential care helps people identify triggers, learn coping tools, understand relapse patterns, and begin repairing the thinking habits that kept addiction going.
A residential day often includes a mix of:
- Individual counseling: One-on-one work on history, motivation, and barriers.
- Group therapy: Practice listening, honesty, accountability, and peer support.
- Education: Learning about cravings, relapse warning signs, and emotional regulation.
- Routine: Sleep, meals, and repetition help the brain settle.
Practical rule: Leaving treatment because someone feels better is not the same as leaving because they're ready.
That point matters because clinical evidence on continuing care indicates that continuing care must extend for a minimum of 3 to 6 months, and up to 12 months may be essential to achieve abstinence rates above approximately 65%. In other words, the strongest gains usually come after the crisis phase, not just during it.
IOP and aftercare test recovery in real life
Intensive Outpatient Programs, often called IOP, are where many people start applying recovery skills at home, at work, or around family stress. This level of care has less protection than residential treatment, but that's also what makes it valuable. Real triggers show up here.
Someone in IOP might attend therapy several days a week while sleeping at home. They may be managing transportation, parenting, or a job while learning how to stay sober in the same environment where use once happened. That takes practice.
A simple way to compare the stages is below:
| Level of care | Main purpose | What it often feels like |
|---|---|---|
| Detox | Physical stabilization | Uncomfortable, fragile, closely monitored |
| Residential | Intensive skill-building and structure | Protected, scheduled, emotionally demanding |
| IOP | Practicing recovery in daily life | Challenging, more independent, real-world |
| Aftercare | Maintaining gains over time | Less intense, but still important |
Aftercare is the longest stage. It can include outpatient therapy, medication management, peer support, sober living, family work, and relapse prevention planning. At this stage, recovery becomes less about surviving treatment and more about building a life that supports sobriety.
How Different Substances Impact Your Recovery Timeline
One reason families get confused is that they hear one person's story and assume it will fit another person's recovery. It usually won't. The substance itself changes the timeline because each drug affects withdrawal, cravings, brain chemistry, and treatment options differently.
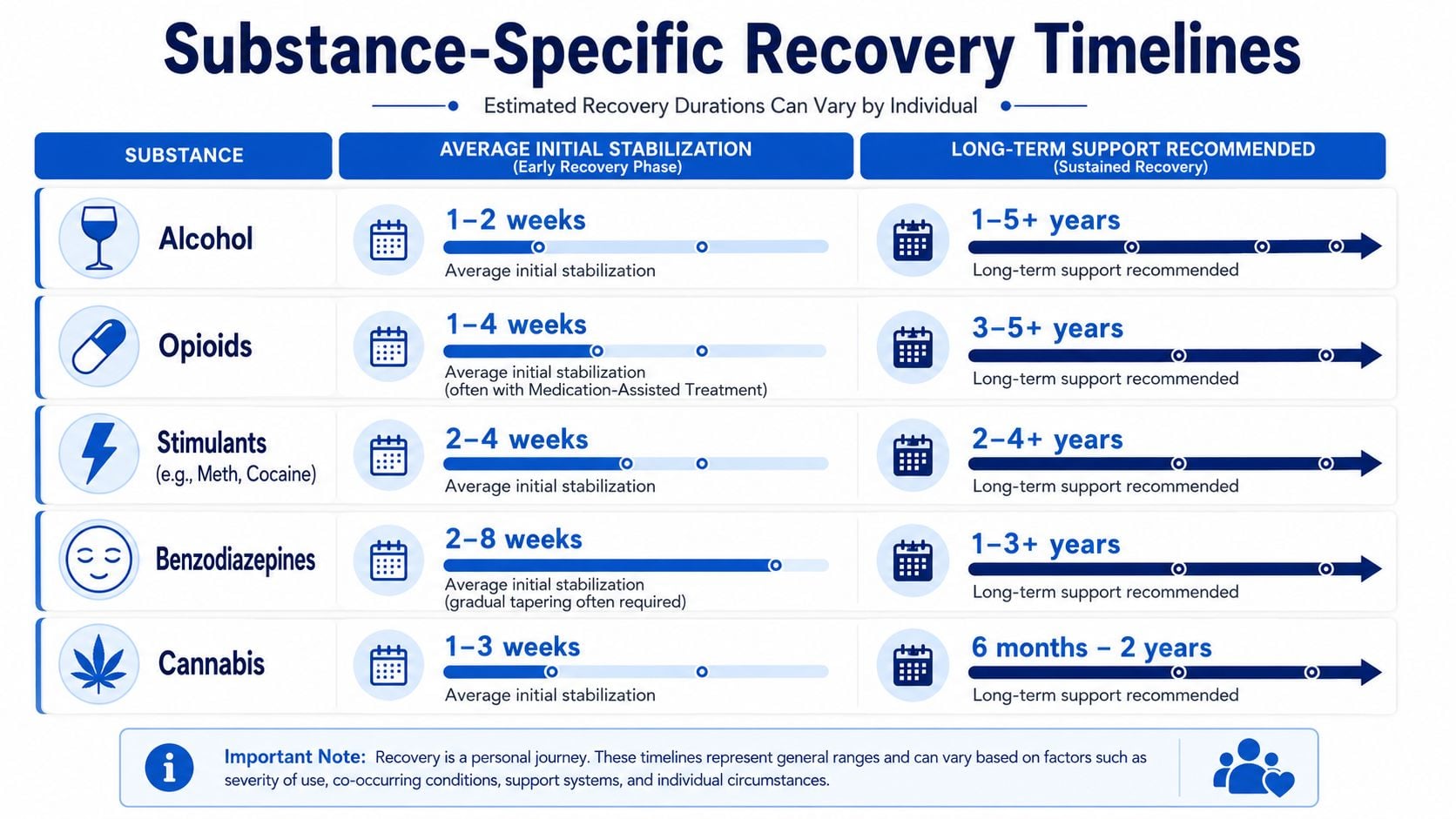
Alcohol recovery often starts differently than opioid recovery
Alcohol can produce dangerous withdrawal, which is one reason medical detox matters. But once that early stage is managed, many people with alcohol use disorder do well with a combination of therapy, support, and in some cases medication. According to recovery rates by drug type, patients treated for alcohol use disorder had the highest one-year recovery success rates at 41%.
That doesn't mean alcohol recovery is easy. It means alcohol treatment outcomes can be stronger than outcomes for some other substances, especially when care is sustained.
Opioid recovery is different. It often involves intense cravings, high overdose risk, and a strong role for medication treatment. The timing of medication can matter a great deal. The ASAM guideline supplement notes that buprenorphine should generally be started at least 6 to 12 hours after the last use of heroin or another short-acting opioid, when mild to moderate withdrawal has begun, to avoid precipitated withdrawal. The same guideline explains that buprenorphine/naloxone and methadone are the primary, most effective treatments for maintaining abstinence in opioid use disorder, outperforming psychological treatment alone, as outlined in the ASAM practice guideline supplement.
Benzodiazepines and stimulants bring different challenges
Benzodiazepine recovery often moves more slowly than families expect. The issue is not just cravings. It is the taper itself. For many people, the safest route is a medically guided reduction rather than a sudden stop.
The same ASAM-linked guidance described above states that slow benzodiazepine tapering, reducing the dose by 25% weekly to 50% of the original dose and then by 12.5% every 4 to 7 days, is successful in two-thirds of patients. That tells families something important. Sometimes "slow" is not a delay. It's the treatment.
Stimulants such as methamphetamine or cocaine can bring a different pattern. Physical withdrawal may look less dramatic than alcohol or benzodiazepine withdrawal, but the emotional crash can be severe. People may struggle with exhaustion, depression, agitation, and powerful urges to use again when energy drops or mood falls.
Here is the key comparison many families need:
- Alcohol use disorder: Often responds well to structured treatment and medications such as oral or monthly injectable naltrexone, which reduce heavy drinking and return to use, with topiramate improving abstinence in some cases, based on the ASAM guidance already noted.
- Opioid use disorder: Often requires longer medication support and careful induction planning.
- Benzodiazepine dependence: Often requires patience and close medical supervision because the taper itself shapes the timeline.
- Stimulant use: Often requires sustained behavioral support because mood, motivation, and craving swings can last beyond the initial crash.
Different substances don't just create different withdrawals. They create different recovery tasks.
Personal Factors That Shape Your Recovery Journey
Two people can enter the same program on the same day and leave with very different needs. Substance use matters, but it isn't the whole story. Recovery also depends on the person carrying it.
Mental health changes the pace
The factor families overlook most often is co-occurring mental health conditions. If someone is recovering from addiction while also living with depression, PTSD, anxiety, or another mental health disorder, the work becomes more layered. They are not just stopping a substance. They are also learning how to handle painful thoughts, sleep disruption, fear responses, panic, shame, or numbness without turning back to use.
According to guidance on brain rewiring after addiction, individuals with co-occurring mental health disorders often require 6 to 12 months longer to achieve stable neural recovery compared to those with a substance use disorder alone. That same source notes that untreated mental illness is a primary driver of longer recovery timelines.
Families can misread the process. A person may look sober but still feel emotionally raw, scattered, or discouraged. That does not always mean treatment isn't working. Sometimes it means deeper issues are finally surfacing.
Life history and support matter too
Other personal factors don't come with neat timelines, but they still matter a lot.
Consider these examples:
- Length and severity of use: A longer and more entrenched pattern usually means more habits, more consequences, and more cues tied to using.
- Physical health: Sleep problems, chronic pain, poor nutrition, and other medical issues can slow progress.
- Home environment: Recovery is harder when alcohol, drugs, conflict, or chaos are still part of daily life.
- Support system: Encouraging family members, sober peers, and steady accountability can help a person stay engaged when motivation dips.
Some people need more time not because they're weaker, but because they're healing more than one wound at once.
A good treatment plan doesn't compare one person to another. It asks a better question. What conditions will give this person the best chance to stay engaged long enough for recovery to take hold?
Key Milestones What to Expect in Early and Long-Term Recovery
Families do better when they know what progress looks like. Recovery milestones are not magic dates, but they can help you recognize normal patterns instead of assuming every difficult week means failure.

The first months feel uneven for a reason
In the first 30 days, many people are still clearing mental fog, sleep disruption, and intense cravings. Some feel relief. Others feel worse before they feel better because emotions that were numbed by substances start coming back.
By around 90 days, routines start to matter more. The person may be attending groups, meeting with a counselor, taking medication as prescribed, and learning how to get through ordinary stress without using. This can also be the stage when confidence rises too fast. Families sometimes hear, "I'm fine now, I don't need all this anymore." That overconfidence can be risky.
By 6 months, the work often gets deeper. The emergency has passed, but grief, relationship damage, guilt, boredom, and identity questions may feel stronger. A person is no longer just trying not to use. They're trying to build a life that makes continued recovery possible.
A simple milestone view can help:
| Milestone | What often happens |
|---|---|
| First month | Withdrawal settles, sleep and mood may still be unstable |
| Around 90 days | Structure and habits begin to form |
| Around 6 months | Deeper emotional work often becomes more important |
| 1 year and beyond | Recovery becomes more lived and less performative |
Long-term recovery gets steadier over time
The larger picture is where many families find hope. According to long-term addiction recovery statistics, less than 20% of patients remain sober for a full year after treatment intake, yet 47% reach at least 12 months of abstinence during the 3 years following treatment. The same source reports a median time from first treatment episode to last use of 9 years.
That tells us recovery is often a long process, not a quick correction.
The same source also notes that for people who achieve 2 years of sobriety, the relapse rate drops to 40%, and the likelihood of sustained sobriety rises substantially after the 5-year milestone. Families should hear that clearly. The early period is often the most vulnerable, but the odds improve with time, especially when the person stays connected to support.
Early recovery asks for persistence. Long-term recovery starts to return stability, trust, and a sense of self.
How Loved Ones Can Support the Recovery Process
Family support can help recovery. Family pressure can also accidentally make it harder. The difference usually comes down to whether support is grounded, informed, and consistent.
Support helps most when it is clear and steady
Loved ones often swing between two extremes. They either try to control everything, or they back away completely because they're exhausted. Neither extreme works well for long.
Helpful support looks more like this:
- Learn the treatment plan: If a doctor recommends medication, tapering, or continuing care, treat that plan seriously.
- Separate support from rescue: Encouragement helps. Covering up consequences often doesn't.
- Expect uneven progress: A rough day, a flat mood, or irritability doesn't always mean relapse is coming.
- Keep boundaries visible: You can love someone and still say no to unsafe behavior in your home.
One strong example comes from benzodiazepine treatment. As noted earlier in the ASAM guideline supplement, slow tapering with specific dose reductions is successful in two-thirds of patients. Families can help by supporting the medical plan rather than pushing the person to "just get it over with." In these situations, patience is part of safety.
What families can do this week
If you want practical steps, start small and stay steady.
- Ask what kind of support helps most right now. Some people need rides, child care, or help with meals. Others need quiet and fewer lectures.
- Join family sessions if they are offered. You may hear the same treatment advice the patient is hearing, which reduces confusion and mixed messages.
- Stop monitoring every mood change. Recovery includes bad days. Watch patterns, not every hour.
- Protect your own stability. Sleep, therapy, support groups, and boundaries matter for families too.
Loving someone in recovery does not mean becoming their doctor, counselor, parole officer, and crisis team all at once.
A healthy family role is powerful because it is steady. You can communicate care, hold limits, and stay aligned with professional guidance without carrying the entire recovery process on your shoulders.
Starting Your Journey Finding Treatment and Navigating Insurance
Starting treatment feels hard mostly because people don't know what happens first. Once that first step is clear, the process becomes much more manageable.
What the first call usually covers
The first call is usually not a test. It is a triage conversation. Staff typically ask what substance is being used, whether the person is currently intoxicated or withdrawing, whether there are mental health concerns, what kind of insurance is available, and whether detox, residential treatment, or outpatient care may be the best fit.
You don't need perfect answers before you call. If all you know is, "Things are getting worse and we need help," that's enough to start.
Questions worth asking a provider include:
- What level of care do you recommend first: Detox, residential, IOP, or standard outpatient?
- How do you handle co-occurring mental health needs: This matters if trauma, depression, or anxiety are in the picture.
- What does family involvement look like: Some programs include family sessions or education.
- Do you offer telehealth options: This can matter for transportation, work, or child care barriers.
If a person also needs counseling support close to home, especially for anxiety, trauma, or relationship strain, a resource such as Penticton mental health support can help families think more broadly about ongoing emotional care beyond the first treatment decision.
How insurance and care planning usually work
Insurance verification is often simpler than people expect. A program can usually check benefits, explain what level of care may be covered, and tell you what authorizations or clinical assessments are needed. The main thing is to call early, before a crisis becomes more dangerous.
For many families, the next step after verification is an assessment. That assessment helps determine whether the safest opening move is detox, whether a residential setting is needed, or whether IOP is appropriate. If the person has military insurance, it also helps to know that some treatment providers welcome TRICARE beneficiaries, which can remove a major barrier for veterans and military families.
A short overview can make the process easier:
| Step | What it usually means |
|---|---|
| Initial call | Share the basics and immediate concerns |
| Insurance check | Confirm benefits and likely options |
| Clinical assessment | Match the person to the right level of care |
| Admission planning | Set timing, paperwork, and next steps |
This short video can help make the first step feel more real and less intimidating.
The most important thing is not choosing the perfect plan on the first try. It is getting a qualified assessment and starting somewhere safe. Recovery rarely begins with certainty. It begins with contact, honesty, and a willingness to accept help.
If you or someone you love is ready to take that first step, Addiction Resource Center LLC offers medically supervised detox with MAT, residential rehabilitation through its partner facility, Ona Treatment Center, and an Intensive Outpatient Program available in person and via telehealth. The team serves adults in Yuba City and Northern California, accepts most major insurance plans, and welcomes TRICARE beneficiaries. You can learn more, schedule a tour, or reach out for guidance at Addiction Resource Center LLC or call and text their 24/7 line at 530-625-7910.