Your phone lights up. It's late. A sibling, partner, or adult child says they used again, or you can hear it in their voice before they admit anything. Your chest tightens. Part of you wants to rush in and fix it. Another part wants to yell, shut down, or ask the question that never helps: …
Your phone lights up. It's late. A sibling, partner, or adult child says they used again, or you can hear it in their voice before they admit anything. Your chest tightens. Part of you wants to rush in and fix it. Another part wants to yell, shut down, or ask the question that never helps: “Why?”
When faced with what to say when someone relapses, you're probably not calm. Most families aren't. They're scared, tired, angry, and trying not to make things worse. The hard truth is that the first words matter, but the timing, tone, and boundaries matter just as much. A perfect script won't rescue a bad moment. A grounded response can keep a bad moment from turning into a worse one.
Table of Contents
- Understanding Relapse Before You Speak
- Your First Response Prioritize Safety and Stay Calm
- How to Open the Conversation With Empathy
- Navigating Difficult Reactions and Denial
- Setting Boundaries to Protect You and Them
- Encouraging Next Steps and Caring for Yourself
Understanding Relapse Before You Speak
A lot of people hear “relapse” and immediately translate it to “everything is ruined.” That reaction is understandable, but it usually leads to the worst possible opening line. Shame makes people hide, minimize, and keep using in secret. A steadier frame gives you a better chance of keeping them engaged.
According to the National Institute on Drug Abuse recovery guidance, relapse rates for substance use disorders are between 40% and 60%, which is similar to other chronic conditions like asthma or diabetes. That doesn't make relapse harmless. It does mean it's common, clinically recognized, and not proof that treatment has failed.

What this changes in real life
If a person had diabetes and their symptoms flared up, you wouldn't call them weak. You'd ask what happened, what changed, and what care is needed now. That same shift helps here. The useful question isn't “How could you do this?” It's “What needs attention right now?”
That frame matters even more for families carrying old hurt. If this isn't the first crisis, your nervous system may already be on high alert. In those moments, it can help to borrow skills from broader family support work around how to assist with mental illness, especially when co-occurring mental health symptoms are part of the picture.
Practical rule: Treat relapse as serious, but don't treat it as a verdict on the person's character.
What works better than panic
Helpful thinking sounds like this:
- “This is a setback.” Serious, yes. Final, no.
- “They may already feel ashamed.” Adding more shame usually shuts the door.
- “My first job is to stabilize the moment.” You can address accountability later.
- “Support and limits can exist together.” Compassion doesn't require pretending everything is fine.
If you ground yourself in that before speaking, your words come out differently. You stop sounding like a prosecutor and start sounding like someone who can help.
Your First Response Prioritize Safety and Stay Calm
In the first minutes, conversation is not the priority. Safety is. If the person is intoxicated, panicked, nodding off, vomiting, confused, shaking, talking about suicide, or unable to stay awake, this is no longer a communication problem. It's a medical and safety problem.
Guidance on helping a loved one who relapsed recommends immediate risk triage after relapse. That means assessing for intoxication, overdose, withdrawal, or suicidal thoughts. Relapse can be medically dangerous, especially when tolerance has changed.
What to do first
Use a simple mental checklist:
- Check responsiveness. Can they answer basic questions? Can they stay awake?
- Look for medical danger. Trouble breathing, severe confusion, chest pain, seizure activity, collapse, or signs that they may have taken more than they can tolerate.
- Ask directly about self-harm. If they sound hopeless, agitated, or detached, ask if they're thinking about hurting themselves.
- Reduce immediate risk. Remove access to substances if you can do so safely. Don't start wrestling with them or turning it into a physical standoff.
- Escalate when needed. If there are signs of overdose, severe withdrawal, or immediate danger, seek emergency medical help.
What not to do in the first hour
People often make the same mistakes when fear takes over. They interrogate, lecture, threaten, or demand promises. None of that helps a person who is impaired, defensive, or medically unstable.
Avoid this in the immediate aftermath:
- Don't demand explanations. You likely won't get the truth if they're intoxicated or scared.
- Don't argue facts. “I know you're high” often becomes a useless fight.
- Don't pile on consequences in the moment. Save major relationship decisions for when everyone is sober and regulated.
- Don't leave safety to chance. If something feels medically wrong, act on that.
If you're deciding between “Am I overreacting?” and “Could this be dangerous?” choose safety.
How to calm yourself enough to be useful
You don't have to feel calm to act calm. Slow your breathing. Lower your voice. Sit instead of pacing if you can. Speak in short sentences.
Try language like:
- “I'm going to stay with you.”
- “I'm focused on making sure you're safe.”
- “We can talk later. Right now I need to know if you need medical help.”
That tone keeps the temperature down. It also protects you from saying the sentence you'll regret tomorrow.
How to Open the Conversation With Empathy
Once the immediate danger has passed, the first conversation should be direct, nonjudgmental, and brief. Clinical guidance on relapse prevention supports a communication style that preserves autonomy. A strong opening is the simple question, “What do you need right now?” followed by listening first and avoiding blame.
That sounds almost too simple, but it works because it does three things at once. It acknowledges reality. It avoids a power struggle. It gives the person a way to speak without defending themselves before they've even started.
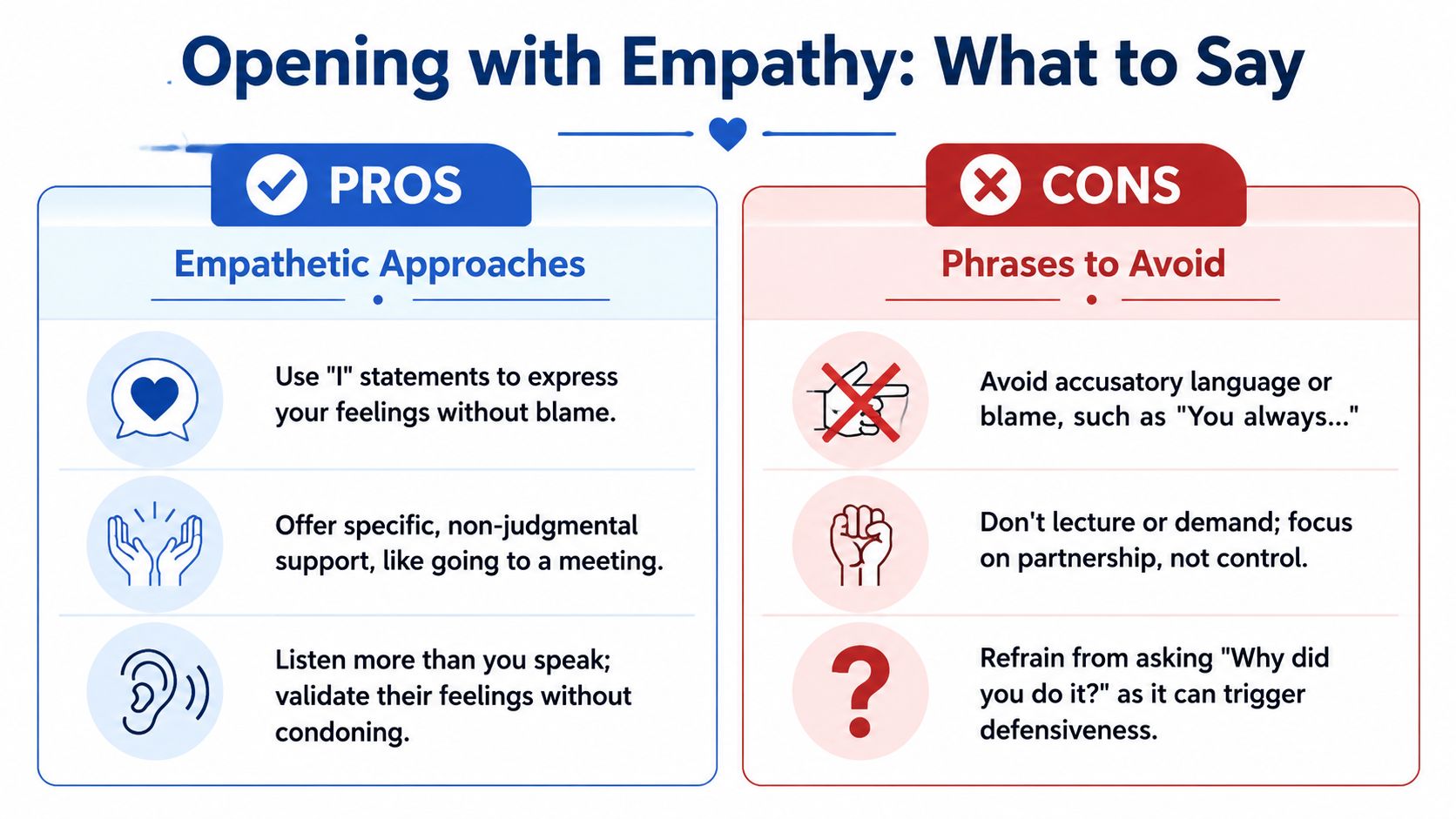
Helpful phrases and harmful ones
| Say this | Not this | Why it works |
|---|---|---|
| “What do you need right now?” | “Why did you do it?” | The first invites honesty. The second invites defense. |
| “I'm glad you told me.” | “I can't believe you did this again.” | It rewards openness instead of punishing disclosure. |
| “We can deal with this one step at a time.” | “You've thrown everything away.” | It keeps the situation grounded and manageable. |
| “I care about you, and I want to understand what happened when you're ready.” | “You always ruin everything.” | It addresses the moment without attacking identity. |
| “This doesn't erase the progress you made.” | “Back to square one.” | It protects motivation, which shame tends to crush. |
Scripts that sound human
If you need actual words, keep them plain:
- For a partner: “I'm upset and I'm also here. I want to help without making this worse.”
- For an adult child: “I love you. I'm not going to shame you. I do need us to deal with this openly.”
- For a sibling or close friend: “You don't have to talk all at once. Start with what you need tonight.”
- For alcohol relapse: “You were sober before. That progress still matters, and you can build from it again.”
For alcohol specifically, some clinical literature has reported relapse rates in the first year after treatment as high as 80%, which supports a response centered on persistence rather than hopelessness. In practice, that means saying, “You became sober before, and you can do it again,” instead of treating the relapse like total erasure.
Phrases that quietly do damage
Some statements feel justified because you're hurt. They still make things worse.
Avoid:
- “How could you do this to me?”
- “I thought you were better.”
- “You just don't want recovery enough.”
- “Promise me this will never happen again.”
These lines push the person toward guilt, lying, or both. If your goal is honest conversation, use language that someone can answer.
Families who want more practice with normalising mental health conversations often find it easier to stay regulated when they've thought through their wording before the next crisis. Preparation helps.
“I'm here to listen, not to win the argument.”
Navigating Difficult Reactions and Denial
The clean scripts above are useful, but they don't work every time. Sometimes the person gets angry. Sometimes they deny the obvious. Sometimes they say you're overreacting, then storm out or shut down. That doesn't mean you failed. It means you're dealing with a person in pain, fear, impairment, or active avoidance.
Guidance on supporting someone through relapse recommends asking, “Would you like to talk about it?” and backing off if the answer is no. That matters because relapse is often a process, not a single event. Timing matters.
When they deny it
Don't get pulled into a courtroom debate. You usually don't need to prove your case.
Try this instead:
- “I'm not going to argue with you. I'm telling you I'm concerned.”
- “You may not want to talk now. I'm available when you're ready to talk openly.”
- “I can see this is escalating. I'm stepping back for now.”
Notice what these lines do. They state reality without cornering the person. They also protect you from the exhausting cycle of accusation, denial, accusation, denial.
When they get angry
Anger often means the person feels exposed, trapped, or ashamed. It doesn't excuse abusive behavior. It does tell you that pushing harder usually backfires.
A few de-escalation rules help:
- Lower the volume. If they raise theirs, don't match it.
- Shorten your sentences. Long explanations sound like lectures.
- Stop trying to get agreement. You only need to communicate your position clearly.
- Leave if needed. A paused conversation is better than a destructive one.
This short video gives a helpful frame for difficult moments with a loved one in relapse:
When the best response is to wait
There are moments when saying less is the right move. If they're intoxicated, actively hostile, or completely shut down, don't force an emotional breakthrough. Save the meaningful conversation for when there's a real chance they can hear you.
Waiting isn't the same as giving up. Sometimes it's the most respectful and effective move available.
Setting Boundaries to Protect You and Them
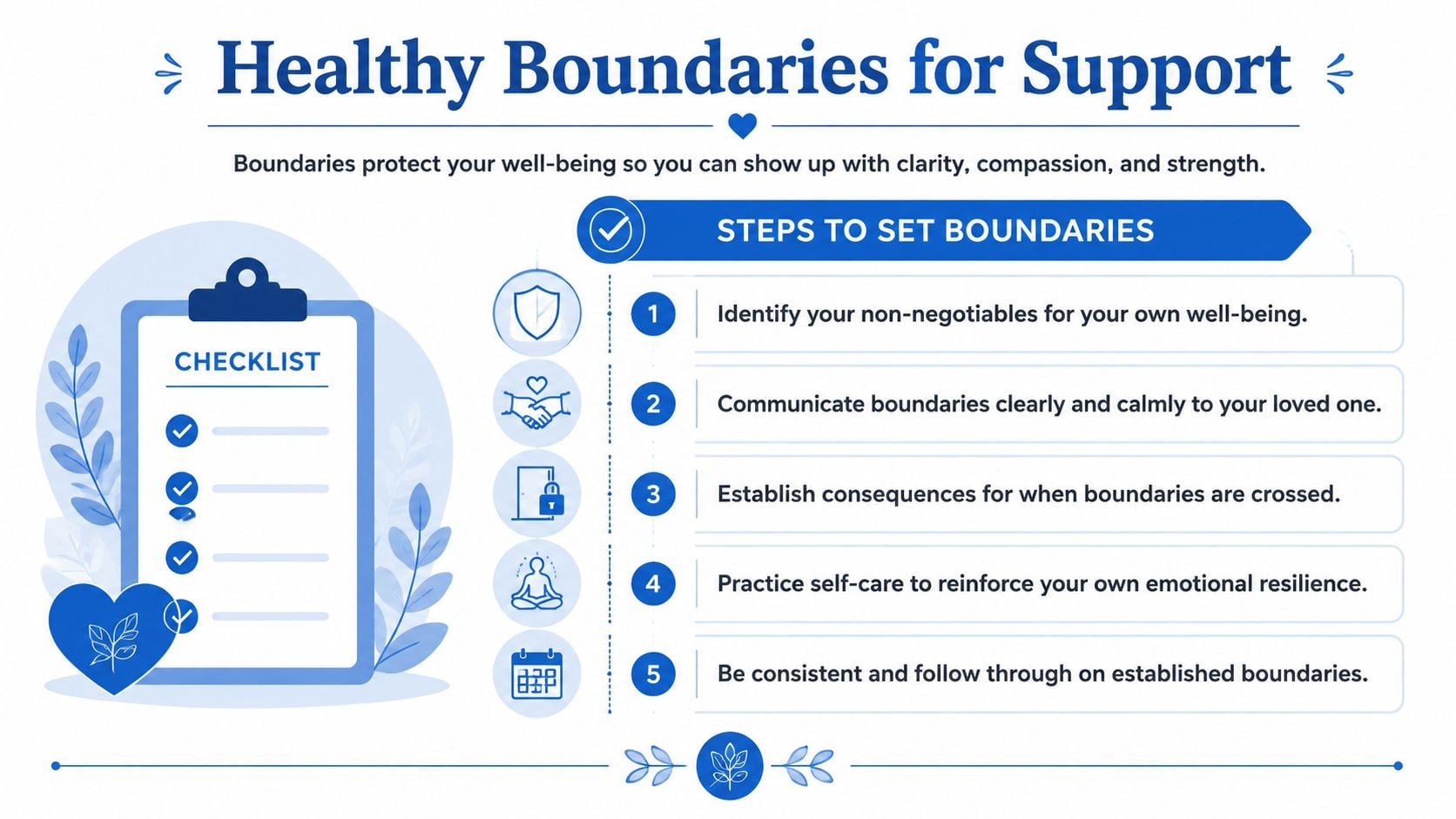
This is the part families often resist, especially if they're scared. They think boundaries will sound cold, or push the person away. In reality, the absence of boundaries usually creates chaos, resentment, and enabling. Clear limits make support believable.
Practical guidance on relapse support emphasizes combining empathy with firm boundaries, including language like “I care about you, and I can't do X while you're using”. That kind of statement preserves dignity because it names care and limit in the same breath.
What a boundary actually is
A boundary is not a threat. It's not a speech designed to control someone into sobriety. It is a clear statement of what you will and won't do.
Examples:
Money
“I won't give you cash. I will help pay for a ride to treatment or a meeting.”Housing
“I care about you. I can't allow substances in this home.”Contact
“I'm willing to talk when you're sober. I'm ending the conversation if you're intoxicated or yelling.”Covering consequences
“I won't call your employer and lie for you.”
Scripts that are firm without being cruel
Many exhausted family members need exact language. Use these if they fit your situation:
- “I love you, and I'm not going to help you stay sick.”
- “I'll help with recovery tasks. I won't help you hide this.”
- “You matter to me. That's why I'm being clear.”
- “I can drive you to an appointment. I can't bring alcohol or drugs into this house.”
- “If you're using, I'm stepping back from this conversation until it's safe and respectful.”
What makes boundaries work
Most boundary failures happen for one of three reasons: the limit was vague, it was announced in anger, or it wasn't followed through. Consistency matters more than perfect wording.
A useful way to think about it:
| Boundary problem | What it sounds like | Better version |
|---|---|---|
| Too vague | “You need to get it together.” | “I won't stay in the room when you're yelling.” |
| Too controlling | “You have to do exactly what I say.” | “Here's what I'm willing to do, and here's what I'm not.” |
| No follow-through | “If this happens again, I'm done.” | “If substances come into the house, you can't stay here tonight.” |
If boundaries are hard for you, a practical guide to setting boundaries can help you think through your firm limits before the next crisis. That's often when people find the words they couldn't access in the moment.
Boundaries protect your sanity. They also stop recovery from becoming everyone else's job except the person using.
Encouraging Next Steps and Caring for Yourself
After the immediate crisis and the first difficult conversation, the next move is simple. Bring the focus back to action. Not punishment. Not endless postmortems. Action.
A practical response after relapse is to review the relapse prevention plan, including triggers, warning signs, and immediate next steps, because earlier intervention gives the best chance of interrupting the process. That may mean contacting a counselor, sponsor, physician, therapist, treatment program, or trusted recovery support the same day.
What to say about next steps
Keep it concrete:
- “What's the next helpful step today?”
- “Do you want me to sit with you while you make the call?”
- “Would it help if I drove you there?”
- “Let's look at what made you vulnerable this time and what needs to change.”
At this point, support becomes practical. You're not trying to manufacture motivation with a speech. You're helping reduce friction so the person can reconnect with care.
Don't disappear from your own life
If you love someone with addiction, exhaustion can sneak up on you. You start managing their moods, tracking their honesty, checking their phone, replaying every conversation, and neglecting your own sleep, meals, work, and relationships. That isn't sustainable.
Your support gets steadier when you have support too. Therapy, Al-Anon, trusted family, faith community, or your own recovery-informed support network can keep you from becoming isolated and reactive. If the relapse is ongoing and the person isn't ready, your job may shift from persuading them to protecting your health and staying available for the next honest opening.
You don't have to choose between compassion and self-respect. The healthiest response usually includes both.
If your loved one needs real help now, Addiction Resource Center LLC offers compassionate substance use treatment in Yuba City, including medically supervised detox with medication-assisted treatment, residential rehab through Ona Treatment Center, and Intensive Outpatient Program options in person and via telehealth. If you're not sure what level of care makes sense, reaching out for guidance can help you take the next step without guessing.