You may be here because methadone helped you get your life back, and now a new question is taking up a lot of mental space. Do I stay on it, or do I try to come off it? For many people, that question carries two very different hopes at the same time. One is the …
You may be here because methadone helped you get your life back, and now a new question is taking up a lot of mental space. Do I stay on it, or do I try to come off it? For many people, that question carries two very different hopes at the same time. One is the hope of living without daily medication. The other is the hope of not losing the stability they worked hard to build.
A family member may be asking a version of the same thing. He's doing better. She's working again. Things are calmer at home. So why not stop now? That sounds simple until you remember what methadone is doing in the background. It isn't just a pill or liquid someone takes each day. For many people with opioid use disorder, it's the medication that reduced cravings, prevented withdrawal, and created enough steadiness to rebuild daily life.
That's why detoxification from methadone should never be treated like a casual next step. It's a medical decision first, and a withdrawal process second. If you do move toward detox, the safest path is usually a slow, supervised taper with a clear plan for what comes after. Alongside medical care, supportive routines like sleep, hydration, gentle movement, and other healthy detox habits can help your body tolerate the process better.
Table of Contents
- Your Guide to Navigating Methadone Detoxification
- Is Detoxing from Methadone the Right Choice for You
- Understanding the Methadone Withdrawal Timeline and Symptoms
- Medically Supervised Tapering The Safest Approach to Detox
- Choosing Your Detox Setting Inpatient vs Outpatient Care
- Beyond Detox Building a Foundation for Long-Term Recovery
- How to Get Help in Yuba City and Northern California
Your Guide to Navigating Methadone Detoxification
A lot of people arrive at this decision during a quiet moment, not a crisis. They're going to work, making appointments, showing up for family, and then the thought appears. Maybe I'm ready for the next chapter. That thought can feel encouraging one day and terrifying the next.
Methadone detoxification brings up mixed emotions because both sides make sense. Wanting to taper off doesn't mean you're ungrateful for the medication. Wanting to stay on methadone doesn't mean you're stuck. It means you're trying to protect your health while thinking carefully about the future.
Why this decision feels so loaded
People often confuse dependence with failure. Those are not the same thing. A body can become physically dependent on a prescribed medication while that medication is still helping the person function, stay safer, and avoid return to illicit opioid use.
That's why the right question usually isn't, “How fast can I get off methadone?” It's, “What choice gives me the best chance of staying healthy, stable, and alive?”
Many patients need permission to say this out loud: “I want off methadone, but I'm scared of what happens if I rush it.”
What families often misunderstand
Loved ones usually see the visible part of recovery. They see school, work, parenting, and calmer behavior. They may not see the daily work that medication is helping support. When families push for a quick detox because things look better, they can accidentally pressure someone into a risky change before that person is clinically ready.
A safer approach is to look at the full picture:
- Current stability: Is the person functioning well day to day?
- Recovery support: Are counseling, recovery meetings, or medical follow-up in place?
- Mental health: Are anxiety, depression, or trauma symptoms manageable?
- Risk of relapse: If cravings return, what protects the person?
Detoxification from methadone can be the right choice for some people. It can also be the wrong choice at the wrong time. Honest timing matters as much as motivation.
Is Detoxing from Methadone the Right Choice for You
For years, many people treated detox as the obvious end goal. If someone was taking methadone, the assumption was that success meant eventually stopping it. Modern addiction care is more careful than that, because long-term outcomes don't always support the idea that detox alone is better.

A major policy milestone came in 1989, when the federal system approved up to 180 days of methadone detoxification for opioid-dependent patients who didn't meet federal guidelines for maintenance or declined maintenance treatment. But a landmark randomized trial found that methadone maintenance performed better than long detoxification. Median treatment retention was 438.5 days for maintenance versus 174.0 days for detoxification, and the maintenance group also had lower heroin-use rates and lower drug-related HIV-risk behavior at 12 months, according to the JAMA trial on methadone maintenance versus long-term detoxification.
Why being medication free is not always the safest goal
That finding helps explain a broader shift in care. In one large U.S. dataset summarized by Recovery Answers, detoxification accounted for 83.7% of treatment episodes in 1994 but 40.5% in 2010. The same summary noted that people who never accessed medication-assisted treatment had a lower probability of successful detoxification with each successive attempt, while longer medication-assisted treatment retention improved with prior detox history. You can read that summary in the Recovery Answers review of repeated detox and medication treatment patterns.
Put plainly, many people do better when treatment stays focused on stability, not on reaching a medication-free status as fast as possible.
That doesn't mean tapering is wrong. It means tapering should have a solid reason behind it.
Questions worth asking before you taper
A useful way to think about this is to separate desire from readiness. You may strongly want to stop methadone and still not be in the best position to do it safely today.
Ask yourself:
- Are you stable in daily life? Work, housing, relationships, and legal stress all affect whether tapering is likely to go smoothly.
- Do you have recovery support outside the clinic? Detox without follow-up leaves a dangerous gap.
- Are you trying to taper for yourself, or to satisfy pressure from others? Pressure from family, employers, or stigma can push people into poor timing.
- Have you discussed maintenance as a valid long-term option? For some patients, continued methadone is the safer and more effective treatment.
Practical rule: If methadone is helping you stay off illicit opioids, think carefully before treating “off medication” as automatically healthier.
People often need help reframing the goal. The goal isn't to prove you can suffer through withdrawal. The goal is recovery that lasts.
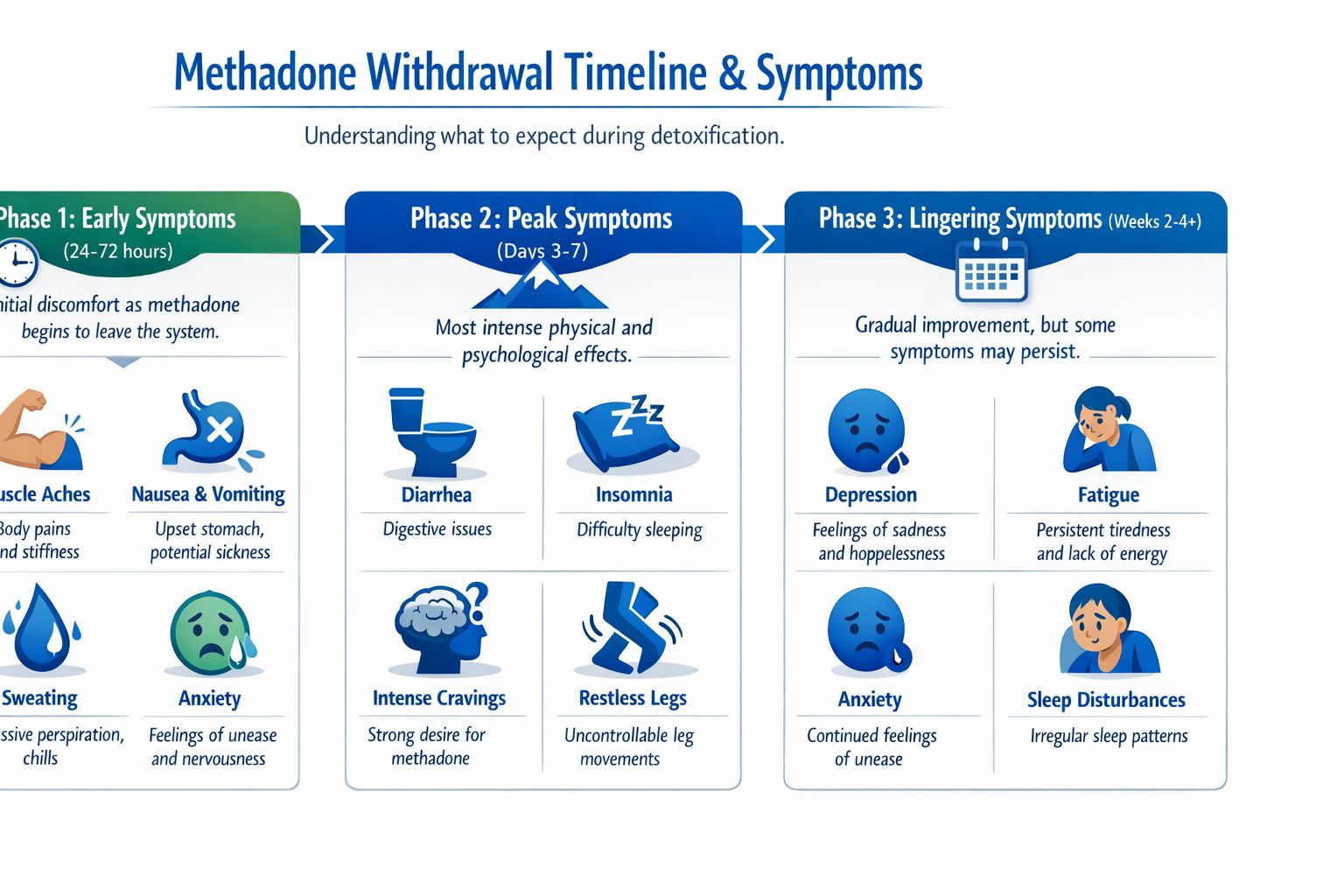
Understanding the Methadone Withdrawal Timeline and Symptoms
Methadone withdrawal confuses people because it doesn't usually behave like withdrawal from a short-acting opioid. Someone may stop or reduce methadone and expect to feel terrible right away. Then little happens at first, and they assume they're in the clear. Later, symptoms build and last much longer than expected.
That delayed pattern happens because methadone stays in the body a long time.
Why methadone withdrawal feels different
Clinical references describe methadone withdrawal as having a longer onset and duration than withdrawal from short-acting opioids. Symptoms may begin within about 24 hours of the last dose, but methadone may take 15 to 60 hours to clear enough to trigger obvious withdrawal, and the overall syndrome is commonly reported to last 3 to 6 weeks, based on the clinical overview at Addiction Center's methadone withdrawal and detox reference.
A simple analogy helps. Withdrawal from a short-acting opioid can feel like falling off a curb. Methadone withdrawal is more like walking down a long staircase in the dark. The drop may not hit all at once, but it keeps going longer than people expect.
Common symptoms families should expect
The symptoms are often a mix of body discomfort and emotional strain. Some are easier to recognize than others.
Common physical and psychological symptoms can include:
- Muscle aches: The body may feel heavy, sore, and flu-like.
- Stomach upset: Nausea, vomiting, cramps, and diarrhea can make hydration difficult.
- Sweating and chills: People may alternate between feeling hot and cold.
- Insomnia: Sleep often becomes fragmented just when the person most needs rest.
- Anxiety and irritability: These can show up early and make everything else feel worse.
- Low mood or depression: This part often worries families because the person may seem discouraged, flat, or hopeless.
- Cravings: The urge to use opioids can return during stress or discomfort.
Withdrawal can also become medically concerning when dehydration, rapid heart rate, hallucinations, or severe depression appear. Those are reasons to involve professionals quickly, not to push through at home.
The hardest part for many families is that the person may look “mostly okay” early on and then feel much worse days later.
Because the timeline is extended, people often need encouragement to pace themselves. A rough day on day four or week two doesn't mean the process is failing. It often means the body is still adjusting.
Medically Supervised Tapering The Safest Approach to Detox
If detoxification from methadone is clinically appropriate, the safest way to do it is usually a slow taper, not abrupt stopping. This is because methadone affects the body over a long period, and the nervous system often reacts badly when the dose drops too fast.
A taper is not about testing someone's toughness. It's about reducing stress on the body and lowering the chance that withdrawal becomes unbearable enough to trigger relapse.
What a taper usually looks like
Clinical references describe methadone detox as a medically supervised process rather than sudden cessation. Doses are often initiated at 10 to 20 mg, increased in 10 mg increments until withdrawal is controlled, then reduced by 10% to 20% per step. When tapering is individualized, schedules may extend from weeks to months. Those details are summarized in the clinical review available through PMC on methadone treatment and detoxification practice.
That kind of pacing gives the care team room to respond to what the patient is experiencing. One person may tolerate a reduction well. Another may develop insomnia, stomach distress, anxiety, or intense cravings and need the taper adjusted.
Why cold turkey causes so many problems
Stopping methadone suddenly can sound appealing because it promises a clean break. In reality, it often creates a long stretch of unnecessary suffering. The person may become exhausted, dehydrated, sleep-deprived, emotionally overwhelmed, or desperate for relief.
Medical supervision helps in several ways:
- Dose changes are controlled. Providers can slow the taper if symptoms become too disruptive.
- Symptoms are treated early. Nausea, diarrhea, sleep problems, and agitation can be addressed before they spiral.
- Mental health is watched closely. Depression and anxiety often intensify during withdrawal.
- Relapse risk is reduced. Structure matters when motivation drops and cravings increase.
A supervised taper can happen in different settings, but the basic principle stays the same. The schedule should fit the patient, not the other way around.
A good taper should be challenging but tolerable. If withdrawal is overwhelming, the plan may be moving too fast.
Choosing Your Detox Setting Inpatient vs Outpatient Care
Once a patient and clinician agree that tapering makes sense, the next question is where detox should happen. This decision shapes how much monitoring, structure, and immediate help the person will have during withdrawal.
For methadone, that choice matters more than many families realize because the process can be prolonged and uneven.
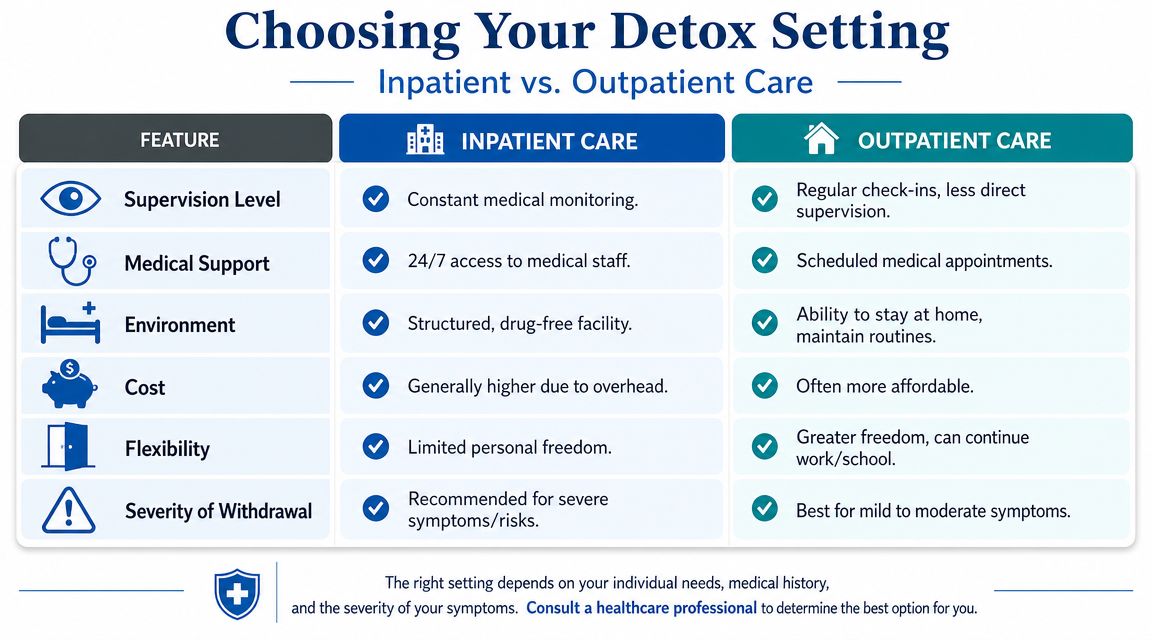
How the two settings differ in real life
Here is a simple side-by-side view.
| Feature | Inpatient Detox | Outpatient Detox |
|---|---|---|
| Supervision | Continuous observation and faster response if symptoms worsen | Scheduled visits or check-ins |
| Medical access | Staff are available throughout the day and night | Support is more limited between appointments |
| Environment | Structured setting away from triggers and easy access to substances | Home setting, which may be supportive or stressful |
| Daily routine | Meals, medications, monitoring, and rest are organized for you | The patient has to manage more of the day independently |
| Best fit | Higher-risk withdrawal, unstable home life, co-occurring problems, or prior relapse | Mild to moderate symptoms with a stable and supportive home |
Outpatient care can work for some people, especially if symptoms are expected to be manageable and the person has reliable transportation, safe housing, and strong follow-up. But outpatient detox asks more of the patient during a time when energy, sleep, and judgment may all be strained.
When inpatient care often makes more sense
Methadone withdrawal has a long time course, and some facilities use inpatient monitoring with symptom-targeted care rather than home detox because supervised settings can adjust taper speed, monitor for severe symptoms such as dehydration, tachycardia, hallucinations, or depression, and reduce relapse risk during the most unstable phase, as described in the earlier clinical discussion of methadone's extended withdrawal pattern.
There is also a practical reason families choose inpatient care. Structured settings remove the daily burden of deciding what to do next when the person feels awful. Instead of guessing, the patient has a team.
Some consumer-facing material claims that fewer than 30% of people complete an unsupervised methadone detox while inpatient completion may be 80% or higher, but that figure is not well-established in neutral public health literature. It appears in a Summer House discussion of inpatient methadone detox, and it's best understood as a sign of a broader evidence gap rather than a settled benchmark.
That said, the clinical logic is still strong. Supervised care tends to give people a better chance because it provides:
- Immediate symptom management: Nausea, diarrhea, insomnia, and distress can be addressed quickly.
- Protection from impulsive relapse: The environment creates space between discomfort and access to opioids.
- Observation by others: Staff can notice dehydration, mental health decline, or exhaustion before the patient asks for help.
- Built-in transition planning: The patient can move directly into continuing treatment instead of going home with no next step.
For a family trying to choose, the key question is not “Which setting is easier?” It's “Which setting matches the actual level of risk?”
Beyond Detox Building a Foundation for Long-Term Recovery
A common scene happens a few days after detox. The hardest physical symptoms have eased, everyone exhales, and the family hopes the problem is over. Then the person goes home to the same stress, the same people, the same habits, and no clear plan for what to do at 7 p.m. when cravings, anxiety, or exhaustion hit.
That is why detox should be viewed as one part of treatment, not the finish line. The body may be clearing methadone, but recovery also has to address judgment, routine, emotional pain, and relapse risk. For some people, this is also the moment to reconsider whether detox was the right step now, or whether continued methadone maintenance with stronger counseling support would better protect stability. Getting off methadone is not the only measure of progress. Staying alive, functional, and engaged in treatment matters more.
What should happen right after detox
The first question after detox is simple. What starts tomorrow?
A good discharge plan fills in that blank before the person leaves care. The next level of treatment might be residential care, a partial hospitalization program, an intensive outpatient program, individual therapy, medication management, peer support, or a combination of these. The goal is to prevent the drop that happens when someone goes from full-time support to too much unstructured time.
The right fit depends on real-life conditions, not wishful thinking. A person with unstable housing, untreated depression, or a pattern of returning to opioid use after short periods of abstinence usually needs more structure. A person with steady housing, reliable transportation, close follow-up, and family support may do well in outpatient care.
What helps recovery last
Recovery after methadone detox works like healing after a major injury. Getting through the acute event matters, but healing holds only if daily support continues while the person is still vulnerable.
Helpful supports often include:
- Counseling: to address cravings, trauma, grief, shame, anxiety, and the habits that kept opioid use going
- Relapse prevention planning: to identify early warning signs and decide in advance what to do when urges rise
- Daily structure: regular sleep, meals, movement, and appointments help the nervous system settle
- Family education: loved ones often need guidance on boundaries, communication, and how to support recovery without trying to control it
- Scheduled follow-up: therapy, medical visits, group sessions, and medication appointments should be arranged before detox ends
One more point often gets missed. If someone completes detox and quickly becomes overwhelmed, that does not mean they have failed. It may mean the level of care was too low, the transition was too abrupt, or methadone maintenance was still the safer clinical choice at this stage.
In Northern California, some families use Addiction Resource Center LLC for medically supervised detox, medication-assisted treatment, intensive outpatient services offered in person and through telehealth, and referral pathways to residential care through a partner facility.
Detox opens the door. Long-term recovery depends on what is built after the door is opened.
How to Get Help in Yuba City and Northern California
If you're trying to decide whether detoxification from methadone is the right move, the next step doesn't have to be a commitment to detox today. The next step can be getting an informed assessment. That conversation should look at your current methadone use, your recovery stability, your medical needs, and whether tapering now is safer than staying on maintenance.
For local families, it helps to see the setting before making a decision.
Practical next steps
If you're in Yuba City or elsewhere in Northern California, keep the process simple:
- Call or text for guidance: Use the 24/7 line at 530-625-7910.
- Ask for an assessment: You can ask whether methadone detox is appropriate now or whether maintenance remains the better option.
- Discuss level of care: Options may include medically supervised detox, residential treatment, or an intensive outpatient program.
- Check practical details: Insurance, including major commercial plans and Tricare, can be reviewed before admission.
- Visit the location: The office is at 1002 Live Oak Blvd., Suite A, Yuba City, CA.
Families often need help understanding what treatment looks like in practice. This short video can make that first call feel less intimidating.
If you're supporting a loved one, you don't need to have the perfect words before reaching out. It's enough to say what's happening now. “They're stable on methadone but want to stop.” “He tried to cut down and feels awful.” “We don't know if detox is even the right idea.” Those are useful starting points.
The safest decision is usually the one based on clinical readiness, not frustration, pressure, or stigma. Sometimes that means a supervised taper. Sometimes it means staying on methadone longer and protecting the progress already made.
If you or someone you love is weighing methadone detox, Addiction Resource Center LLC can help you sort out the primary question first: whether detox is appropriate now, and what level of care makes sense if it is. Their team in Yuba City offers medically supervised detox with MAT, IOP in person and by telehealth, and access to residential care. You can call or text 530-625-7910 any time to ask questions, verify insurance, or talk through options privately.