Explore co-occurring disorder treatment through integrated care that heals both mental and physical health challenges simultaneously.

Having both a mental health condition and a substance use disorder at the same time is more common than you might think. When these conditions occur together, treating them separately rarely works.
At Addiction Resource Center, we’ve seen firsthand how co-occurring disorder treatment works best when it addresses both the mind and body at once. This blog post walks you through what integrated care looks like and how to find it.
What Co-occurring Disorders Really Look Like
About 21.2 million adults in the United States have both a mental illness and a substance use disorder simultaneously, according to SAMHSA’s 2024 National Survey on Drug Use and Health. That’s nearly one in ten American adults. Co-occurring disorders mean a person has a diagnosed mental health condition like depression, anxiety, PTSD, or bipolar disorder happening at the same time as a substance use disorder. The combination isn’t random. Anxiety and mood disorders show up frequently alongside alcohol and opioid misuse. Someone might use alcohol to quiet racing thoughts from an anxiety disorder, or rely on stimulants to manage depression symptoms.
The Feedback Loop That Worsens Both Conditions
The relationship between these conditions creates a feedback loop where one makes the other worse. Untreated anxiety drives someone toward alcohol for relief. That alcohol use then damages sleep and mood, which intensifies the anxiety. Treating just the addiction without addressing the underlying mental health issue sets someone up for failure. The person stays anxious or depressed, the cravings return, and relapse becomes almost inevitable.
Why Separate Treatment Programs Don’t Work
Traditional addiction treatment programs focus almost entirely on substance use. Mental health clinics focus on psychiatric symptoms. This split approach leaves gaps.
A person in a standard addiction program might receive group therapy and medication for cravings, but their untreated depression goes nowhere. They complete the program technically sober but still deeply depressed. Within months, they return to using.
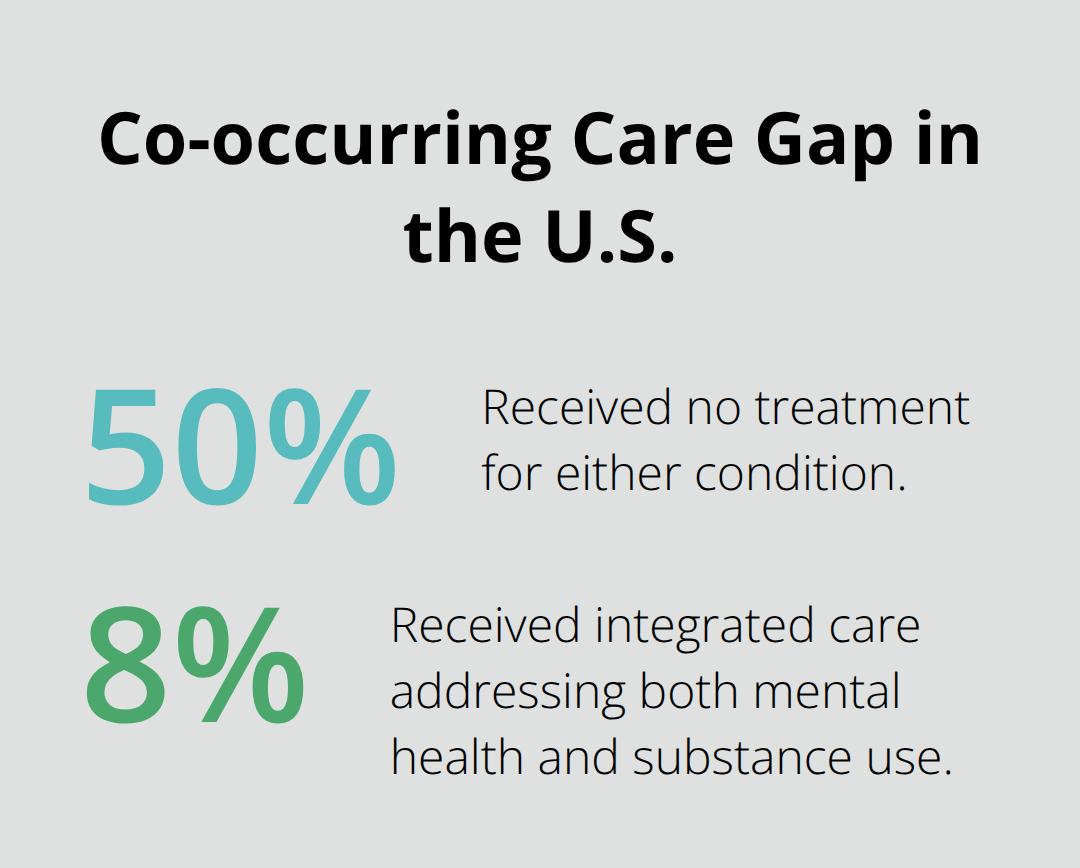
Research shows that when people with co-occurring disorders receive treatment for only one condition, outcomes are poor. Of those with co-occurring disorders, half received no treatment at all, and only 8 percent received care addressing both their mental health and substance use issues simultaneously. The numbers tell the story clearly.
What Integrated Care Achieves
Integrated care that treats both conditions at once produces measurably better results in housing stability, employment, hospitalization rates, and long-term abstinence. Programs using integrated approaches see clients stay in treatment longer, achieve better psychiatric outcomes, and maintain recovery more consistently than those using siloed models. This difference matters because it reflects real lives changed-people who find stable housing, return to work, and build sustainable recovery rather than cycling through repeated relapses.
Understanding why co-occurring disorders demand simultaneous treatment sets the stage for exploring how integrated programs actually work and what makes them effective.
How Integrated Programs Actually Treat Co-occurring Disorders
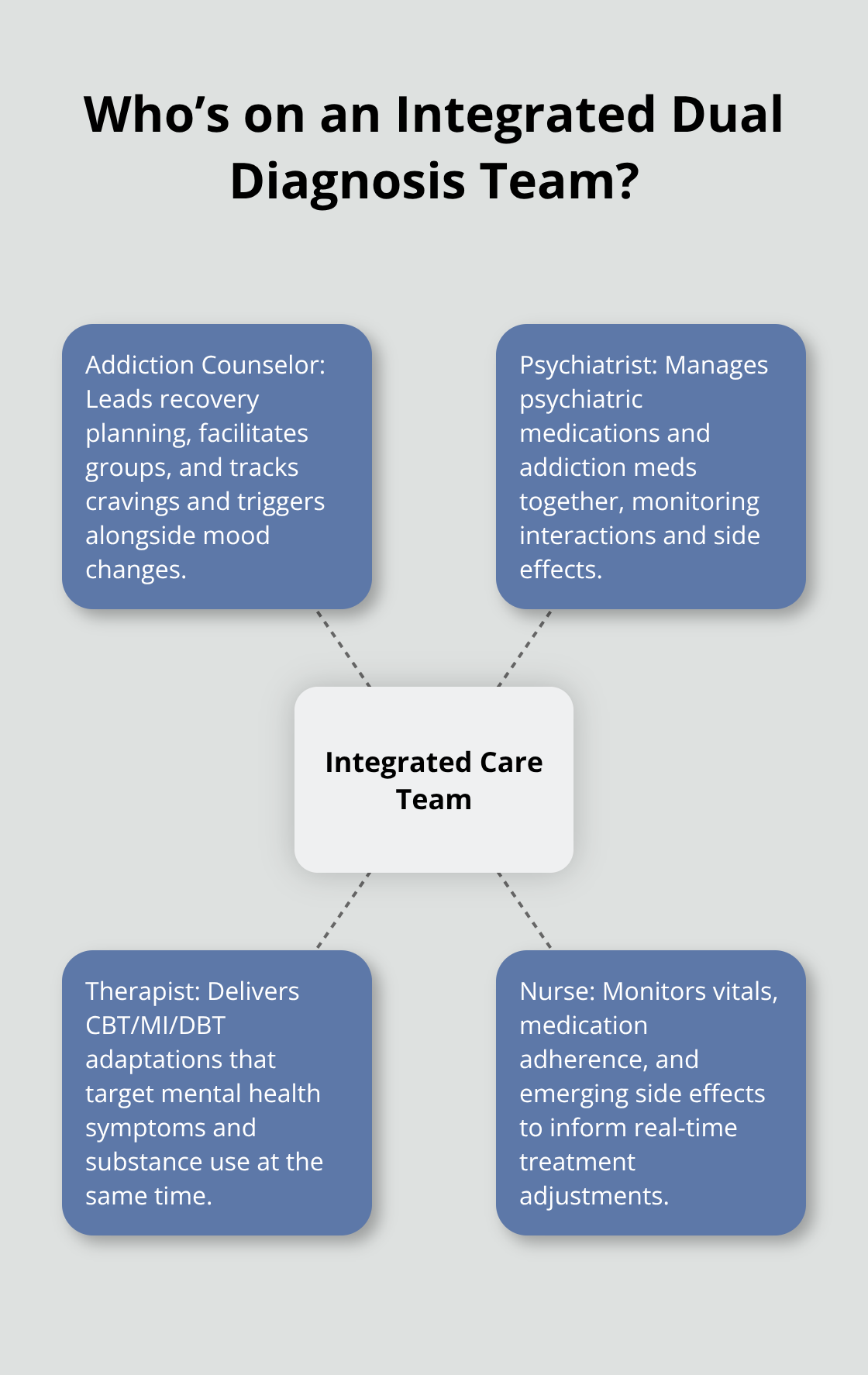
Integrated dual diagnosis programs operate fundamentally differently from traditional addiction or mental health clinics. Instead of referring clients between separate departments, integrated programs assign a single treatment team that includes addiction counselors, psychiatrists, therapists, and nurses working together on one coordinated plan. Each team member sees the same client and participates in the same treatment meetings.
This structure eliminates the common problem where a client receives conflicting advice from different providers or falls through cracks between systems.
The team meets regularly to discuss progress, adjust medications, modify therapy approaches, and solve problems as they emerge. Research published in peer-reviewed journals shows that integrated programs produce measurably superior outcomes compared to coordinated or co-located models. Clients in fully integrated programs stay in treatment longer, achieve better abstinence rates, experience fewer hospitalizations, and report higher satisfaction with care. Programs that use what researchers call the coordinated model-where providers simply communicate with each other but work separately-show weaker results than programs where clinicians actually sit in the same room making decisions together.
Evidence-Based Therapies That Address Both Conditions Simultaneously
Cognitive Behavioral Therapy remains the strongest evidence-based approach for co-occurring disorders when delivered with specific adaptations. Standard CBT teaches clients to identify thought patterns driving both substance use and mental health symptoms, then practice new responses. For co-occurring work, therapists modify this to address triggers that activate both conditions simultaneously. A client with depression and alcohol use disorder learns to recognize how negative thoughts create emotional pain, which then creates craving for alcohol as pain relief. The therapy directly targets that chain.
Motivational Interviewing works particularly well for ambivalence about treatment. Many people with co-occurring disorders feel torn between wanting recovery and fearing the withdrawal or emotional pain involved. Skilled motivational interviewing helps clients resolve this ambivalence rather than pushing them toward change. Family involvement in therapy produces stronger outcomes than individual therapy alone, according to research by Kelly and Daley published in addiction treatment literature. When family members understand the co-occurring conditions and learn how to respond supportively without enabling, relapse rates drop noticeably.
Dialectical Behavior Therapy addresses the emotional dysregulation common in co-occurring presentations, particularly for clients with trauma histories or borderline personality features alongside substance use. This approach teaches clients to tolerate distress without turning to substances while simultaneously working on changing problematic patterns.
Medication Management as Part of the Treatment Team
Medication in integrated care requires close coordination that standard addiction programs cannot provide. The psychiatrist must monitor how medications for depression or anxiety interact with the client’s substance of choice and with any medications used for addiction treatment. Benzodiazepines like Xanax or Valium, commonly prescribed for anxiety, carry serious risks when combined with opioids or alcohol. An integrated team catches this problem immediately.
Medications for substance use disorders themselves require psychiatric oversight. Naltrexone, used for both alcohol and opioid use disorders, can trigger or worsen depression in some clients. Buprenorphine, the gold standard for opioid use disorder treatment, requires careful dosing and monitoring for interactions with psychiatric medications. In non-integrated settings, the addiction counselor and the psychiatrist never discuss these concerns. In integrated programs, the team adjusts medications based on real-time feedback about mood, cravings, side effects, and substance use patterns.
Medication combined with psychotherapy produces significantly better outcomes than either treatment alone for co-occurring disorders. The medication addresses the biological drivers while therapy addresses the behavioral and cognitive patterns. Neither alone proves sufficient.
How Treatment Teams Coordinate Care
Integrated programs establish clear communication protocols that keep all providers aligned. When a client reports increased anxiety during a therapy session, the therapist immediately alerts the psychiatrist. When medication adjustments occur, the counselor monitors how these changes affect cravings and mood in group sessions. This real-time feedback loop prevents the delays and miscommunications that plague traditional systems.
The team also coordinates around relapse risk. If a client shows signs of increased substance use, the psychiatrist checks whether medication side effects or dosing problems contributed to the problem. The therapist explores whether new stressors or untreated trauma symptoms triggered the relapse. The counselor examines whether the client’s support network weakened. This multidisciplinary perspective catches problems that single-discipline providers would miss.
Understanding how integrated programs structure their treatment teams and coordinate care across disciplines reveals why these approaches work. Tailored treatment plans ensure that generic approaches don’t fragment care, strengthening the foundation for lasting recovery. The next section explores the practical steps you can take to find a program that delivers this level of coordinated, evidence-based treatment.
Practical Steps to Find Quality Co-occurring Disorder Treatment
Ask about true integration, Not Just Coordination
Finding a program that actually delivers integrated care requires asking specific questions most people don’t know to ask. Start by asking whether the program employs psychiatrists or psychiatric nurse practitioners who work directly with addiction counselors on the same treatment team, not in separate departments. Ask how often the treatment team meets to discuss individual clients and whether psychiatrists attend these meetings regularly. Many programs claim integration but actually operate coordinated care, where a therapist and psychiatrist exist in the same building but rarely communicate.
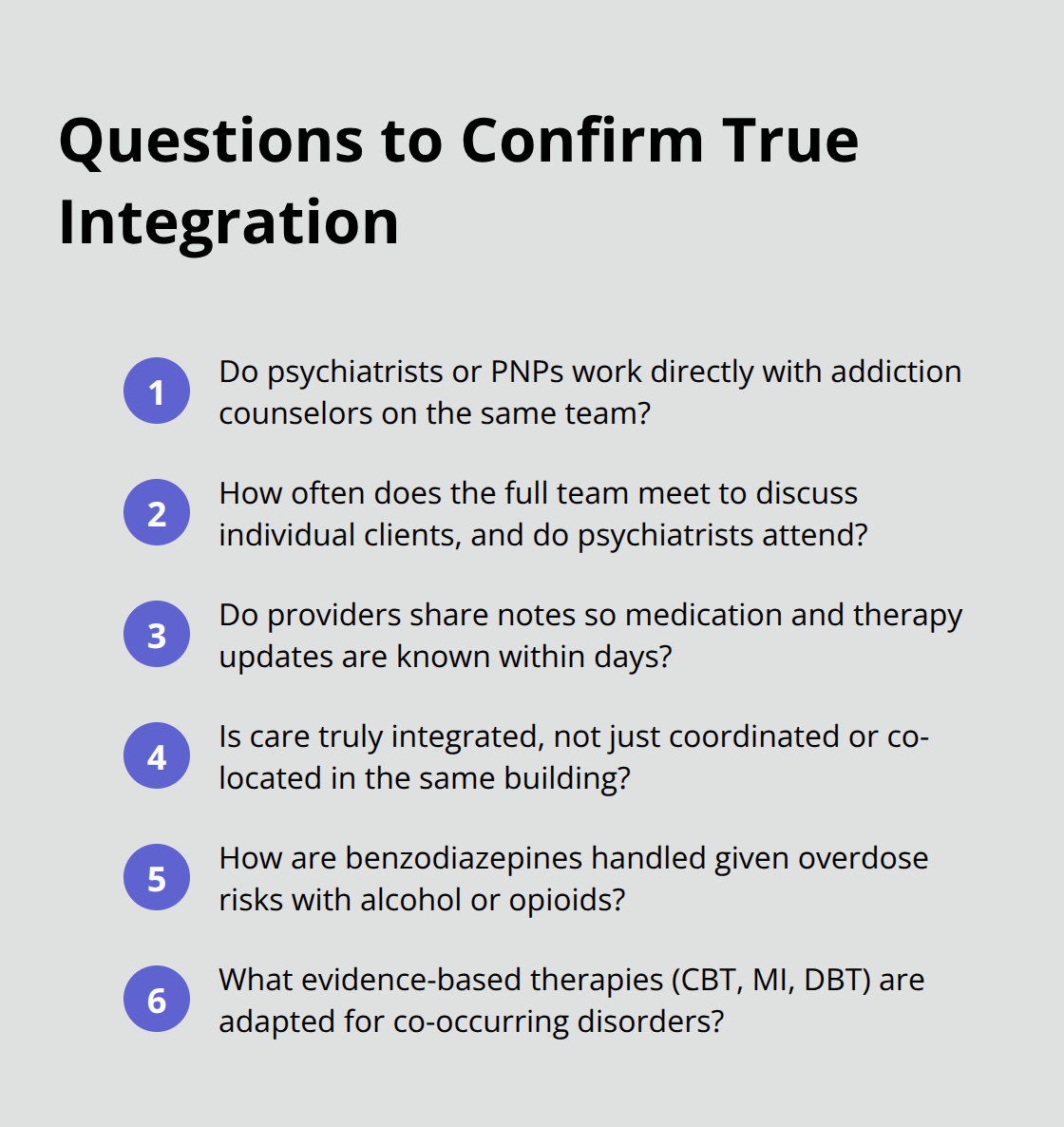
Real integration means the psychiatrist knows your therapy progress and the therapist knows your medication side effects within days, not weeks. Ask the program directly: does the psychiatrist review therapy notes and does the therapist attend medication management appointments? If the answer is vague or no, the program isn’t truly integrated. Also ask about their approach to benzodiazepines. Programs that readily prescribe Xanax or Valium alongside addiction treatment demonstrate they don’t understand co-occurring care, since these medications carry serious overdose risks when combined with opioids or alcohol. Strong integrated programs use safer alternatives like buspiron for anxiety or SSRIs for both anxiety and depression.
Evaluate Evidence-Based Treatment and Outcomes
Ask what evidence-based therapies they offer and whether therapists have specific training in cognitive behavioral therapy or motivational interviewing adapted for co-occurring disorders, not just general addiction counseling. Request their relapse rates and treatment completion rates, then compare across programs. Programs willing to share these numbers tend to have better outcomes than those that deflect the question.
What separates comprehensive programs from mediocre ones often comes down to how thoroughly they assess your specific situation before treatment starts. A quality program conducts detailed assessments that examine not just substance use and psychiatric symptoms but also trauma history, medical conditions, family dynamics, employment status, and housing stability. Research shows that housing and employment stability directly predict treatment success, yet many programs ignore these factors entirely.
Assess Comprehensive Support Services
Ask whether the program connects clients to housing assistance, employment counseling, or vocational rehabilitation as part of treatment, not as an afterthought. Ask specifically about their approach to medication-assisted treatment if you have opioid use disorder. Buprenorphine combined with counseling produces superior outcomes compared to abstinence-only approaches. Programs that dismiss medication-assisted treatment or treat it as a last resort rather than a first-line option are limiting your chances.
Your treatment plan should address your specific combination of disorders, your trauma history, your family situation, and your recovery goals. Ask whether the program offers family therapy or family education sessions, since research demonstrates that family involvement significantly improves outcomes. Ask whether the program has peer support specialists with lived experience of co-occurring disorders on staff, not just credentialed clinicians. Peer support specialists who have recovered from dual diagnosis understand recovery differently than clinicians without personal experience and often connect with clients more authentically.
Final Thoughts
Integrated co-occurring disorder treatment addresses both conditions simultaneously rather than hoping one improves while ignoring the other. The evidence proves that people who receive integrated care stay in treatment longer, maintain abstinence more consistently, experience fewer hospitalizations, and report higher quality of life than those receiving fragmented treatment. When a therapist understands your depression and your addiction counselor knows your medication side effects, recovery becomes possible in ways that separate treatment never achieves.
Taking the first step toward recovery starts with recognizing that you deserve treatment designed for your specific situation, not a generic program that treats addiction and mental health as separate problems. Call a program and ask the hard questions: Does their psychiatrist work directly with their counselors? Do they offer evidence-based therapies like cognitive behavioral therapy adapted for co-occurring disorders? Will they connect you to housing and employment support? Your answers determine whether you’re entering truly integrated care or settling for coordination that leaves gaps.
We at Addiction Resource Center understand that co-occurring disorder treatment requires more than standard addiction programs provide. Our team of professionals delivers personalized treatment that addresses both your mental health and substance use needs through integrated outpatient programs tailored to your recovery goals.