You may be reading this in a tense moment. Maybe detox just ended, and home suddenly feels both comforting and risky. Maybe weekly therapy isn't enough anymore, but the thought of moving into residential treatment feels too disruptive, too expensive, or not necessary. Families often land here with the same question: "Is there something in …
You may be reading this in a tense moment. Maybe detox just ended, and home suddenly feels both comforting and risky. Maybe weekly therapy isn't enough anymore, but the thought of moving into residential treatment feels too disruptive, too expensive, or not necessary. Families often land here with the same question: "Is there something in between?"
There is. A partial hospitalization program rehab option is often the middle ground people need when recovery requires real structure, but not round-the-clock living at a facility. It gives someone a strong clinical routine during the day and lets them return home at night. For many people, that balance matters. They can keep sleeping in their own bed, stay connected to family, and still receive a high level of support.
It's similar to using a walking boot after an injury. You aren't in the emergency room anymore, but you also aren't ready to run without support. Recovery can work the same way. Some people need more than check-ins and good intentions. They need daily therapy, close monitoring, skill-building, and a plan for getting through evenings without slipping back into old patterns.
That doesn't mean they're failing. It usually means they're being honest about the level of help needed right now.
Table of Contents
- Introduction The Crossroads of Recovery
- What Is a Partial Hospitalization Program
- A Day in the Life The Structure of PHP Rehab
- PHP vs IOP vs Residential Treatment
- Navigating Cost Insurance and TRICARE for PHP
- Finding the Right PHP Questions to Ask Providers
- Your Next Step to Recovery in Northern California
Introduction The Crossroads of Recovery
A lot of people arrive at this point after doing something hard already. They may have stopped using, made it through withdrawal, or admitted that life has become unmanageable. Then comes the next challenge. Staying sober isn't just about stopping. It's about building enough support around the person so they can keep going when stress, shame, cravings, conflict, and exhaustion all show up at once.
Families often get confused by the treatment language. Inpatient. Outpatient. Intensive outpatient. Partial hospitalization. The terms can sound clinical and cold, especially when you're trying to make a decision quickly. But underneath the jargon is a simple question: how much structure does this person need to stay safe and keep moving forward?
PHP often enters the conversation when someone needs more than a weekly appointment or an evening group. They may be emotionally raw after detox. They may have relapsed while trying a lower level of care. They may also be dealing with anxiety, depression, trauma symptoms, or family stress that makes early recovery feel fragile.
Sometimes the right level of care isn't the most restrictive one. It's the one that gives enough support to hold the day together.
That is why PHP can be such a relief to hear about. It offers a serious treatment schedule without requiring twenty-four-hour residential living. Someone can spend the day focused on recovery and then practice those skills in real life each evening. That matters because recovery doesn't happen in a bubble. It happens at home, at dinner, during arguments, in lonely hours, and on the drive past familiar triggers.
For many families, PHP isn't a last resort. It's a smart fit.
What Is a Partial Hospitalization Program
A partial hospitalization program, or PHP, is a high-support outpatient level of care for people who need treatment for much of the day but do not need to stay overnight in a facility. The person attends structured clinical care during the day, then returns home or to supportive housing in the evening.

Why people call it a bridge
Families often hear the word "hospitalization" and assume it means sleeping at the treatment center. In PHP, that is not what usually happens. The "hospital" part points to the intensity and clinical oversight, not to round-the-clock living on site.
A simpler way to understand it is this: PHP gives a person a strong daytime container for recovery. Hours that might otherwise feel risky or unstructured are filled with therapy, skill practice, medical or psychiatric check-ins, and support from a treatment team. Then the person goes home and tests those recovery skills in ordinary life, where real stress tends to show up.
That is why people often describe PHP as a bridge. It connects two needs that can feel hard to balance at the same time. A person may need serious help and close monitoring, but still be stable enough to sleep at home, see family, and begin rebuilding daily routines outside a residential setting.
Who it usually fits
PHP often fits people who are medically stable enough to live outside a facility but still need frequent clinical support to stay steady in early recovery. That might include someone leaving detox or inpatient treatment, someone who relapsed in a less structured program, or someone dealing with both substance use and mental health symptoms at the same time.
It can also be a practical option for families trying to answer two questions at once: "How much help does this person need?" and "Can we realistically manage the logistics?" PHP allows people to receive intensive care without the full disruption of moving into residential treatment.
- People stepping down from detox or inpatient care who still need a high level of structure
- Adults with high relapse risk during long stretches of unstructured time
- People with co-occurring mental health concerns who may need therapy plus psychiatric support
- Families looking for serious treatment with nights at home when that home setting is safe and supportive
Practical rule: PHP is often considered when someone needs daily treatment and close support, but does not need twenty-four-hour supervision.
Why it feels different from standard outpatient care
Weekly counseling can help, but recovery often becomes unstable in the long space between appointments. PHP tightens that gap. The schedule creates repetition, accountability, and faster response when cravings, mood changes, sleep problems, or family stress start building.
There is also a practical side that families ask about early. PHP is often less expensive than residential treatment because it does not include overnight housing, meals, and round-the-clock staffing. Exact costs vary by program, location, insurance coverage, and how many services are included, which is why benefit verification matters before admission.
In plain terms, PHP sits in the middle. It offers more structure than standard outpatient care and more day-to-day independence than residential rehab. For many people, that middle ground is what makes treatment feel possible.
A Day in the Life The Structure of PHP Rehab
At 7:30 in the morning, a parent may be helping someone find car keys, refill a water bottle, and brace for a full treatment day. By dinner, that same person is back home, tired, a little raw, and carrying new coping tools that still need practice. That daily rhythm is what makes PHP easier to understand. It is intensive during the day, then real life resumes at night.
For families, the schedule often answers the biggest question. What happens there? The short answer is that PHP fills the day with treatment on purpose. Recovery tends to wobble when too many hours are left open, especially early on. A steady routine gives the brain and body something they may not have had in a while: predictability.
A typical day often starts with a check-in. Staff may ask about cravings, sleep, medication side effects, mood, conflict at home, or what happened after yesterday's session ended. That may sound simple, but it serves an important job. It helps the team catch problems early, while they are still manageable.

What the day can include
No two programs use the exact same schedule, but many PHPs build the day from the same core pieces:
- Morning group therapy focused on triggers, shame, isolation, conflict, or the stress of early recovery
- Individual counseling to work through personal history, current obstacles, and treatment goals
- Skill-building sessions that teach practical tools from CBT or DBT for thoughts, emotions, and urges
- Medication management with a prescriber or nurse to review benefits, side effects, and consistency
- Relapse prevention planning that turns general intentions into specific steps for high-risk situations
- Family sessions to address trust, communication, boundaries, and the strain addiction places on a household
A good way to picture it is a rehab day that works like physical therapy after an injury. The exercises may not feel natural right away, and some days feel repetitive, but repetition is part of how healing takes hold. In PHP, people are not only talking about change. They are practicing it, several times in one day, with support close by.
The day also has a practical side that families appreciate once treatment begins. Meals, transportation timing, medication refills, work leave, and child care do not disappear because someone enters rehab. A well-run PHP helps families handle those details, because missed rides or medication problems can affect treatment just as much as motivation can.
The visual below helps show how that structure often flows across a treatment day.
Why evenings still matter
The hours after PHP are part of treatment too.
Going home each night gives a person the chance to use new skills in the setting where recovery has to work. That can be encouraging, but it can also be hard. Home may include tension with a partner, access to alcohol, old routines, or the loneliness that hits after the busy part of the day ends.
That is why discharge planning does not wait until the last week. Strong programs help patients map out evenings early. Who is picking them up? What is the dinner plan? What happens between 6 p.m. and bedtime? If cravings rise, who gets the call? Families often feel relief when those questions are addressed directly, because recovery becomes less abstract and more manageable.
A person does not need a perfect home to succeed in PHP. They do need a setting that is safe enough for the level of care, plus a realistic plan for the hours treatment is over.
A strong PHP asks what happened in therapy today and what is likely to happen tonight when stress returns.
In-person and virtual options
Some programs are in person only. Some offer virtual PHP, or a mix of both, for people who face transportation problems, health limitations, work disruptions, or caregiving demands. The format matters less than whether the person can attend consistently, stay engaged, and get the right level of clinical support.
For many families, that flexibility can make treatment possible. The best next question is usually not which format sounds better on paper. It is which format this person can realistically show up for, day after day, while recovery is still fragile.
PHP vs IOP vs Residential Treatment
Families often compare levels of care the way they compare schools or hospitals. They want a simple answer. Which one is best? The harder truth is that the best option depends on the person's stability, living situation, relapse risk, and need for supervision.
Residential treatment offers the most containment. The person lives at the facility and receives care in a fully immersive setting. PHP keeps the intensity high during the day but sends the person home at night. Intensive outpatient, or IOP, is lighter and usually works better when someone already has a bit more stability and can handle longer periods of independence.
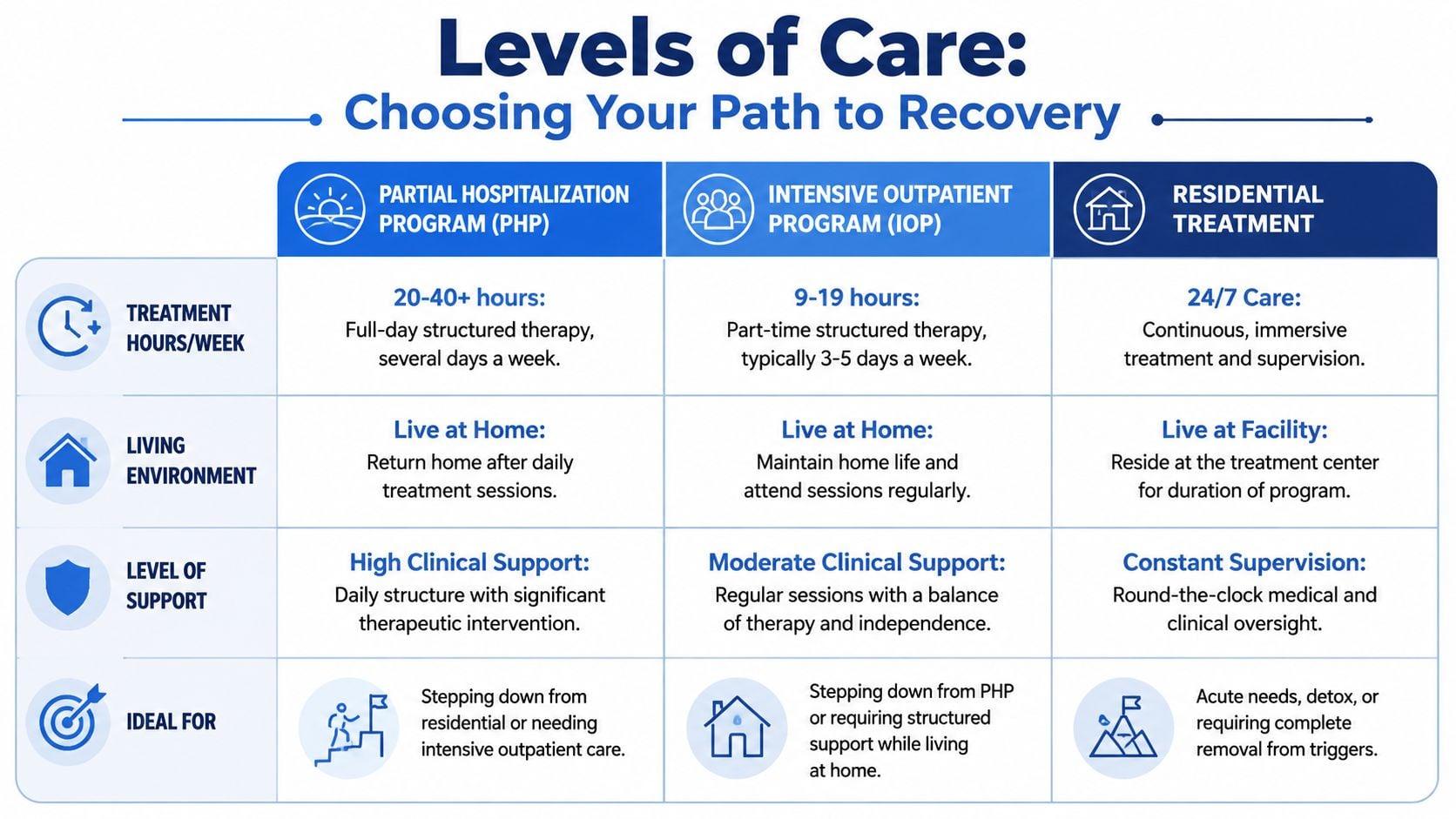
Treatment Level Comparison PHP vs IOP vs Residential
| Feature | Partial Hospitalization (PHP) | Intensive Outpatient (IOP) | Residential Rehab |
|---|---|---|---|
| Time commitment | Most of the day, several days a week | Fewer hours, often built around work or home life | Full-time living at the facility |
| Living arrangement | Lives at home or in supportive housing | Lives at home | Lives at the treatment center |
| Clinical support | High outpatient structure with frequent therapeutic contact | Moderate structure with more independence | Highest level of daily supervision |
| Best fit | Needs strong daily support without 24/7 housing | Can manage more free time between sessions | Needs constant monitoring or separation from triggers |
| Home environment matters | Yes, because the person returns home nightly | Yes, often even more | Less immediately, because care happens on site |
How to think about the choice
A simple way to sort through the options is to ask where the biggest risk sits.
If the danger is medical instability, severe withdrawal risk, or the inability to stay safe outside a controlled setting, residential care may make more sense. If the danger is unstructured time, emotional volatility, repeated relapse after lower-intensity care, or needing daily accountability, PHP often becomes the better fit. If someone is motivated, stable, and able to practice recovery skills with fewer touchpoints, IOP may be enough.
Here are a few examples:
Stepping down after inpatient care
Someone may no longer need overnight supervision, but still feels shaky. PHP can preserve momentum without the abrupt drop to only a few treatment sessions each week.Trying to avoid another relapse
A person may be living at home, going to work inconsistently, and white-knuckling evenings. In that case, IOP may feel too loose, while PHP gives the day stronger boundaries.Needing complete separation from the environment
If home is chaotic, unsafe, or tied tightly to active use, sending someone back there every night may work against recovery. Residential treatment may be the safer call.
The right level of care should match the person's real life, not the version of life everyone wishes they had.
Cost and disruption matter too
Clinical need comes first, but practical life matters. Residential treatment often disrupts work, parenting, transportation, and daily responsibilities more heavily because the person lives away from home. PHP can reduce some of that disruption while still providing a strong schedule. IOP usually offers the most flexibility, but flexibility only helps when the person can safely use it.
That is why level-of-care decisions should never be based on pride alone. "I should be able to do less" is not a treatment plan. The better question is, "What level gives me the best chance to stay engaged and keep building recovery?"
Navigating Cost Insurance and TRICARE for PHP
Money stress can stop families from making calls. People worry that treatment will be unaffordable, that insurance will deny care, or that they'll agree to something without understanding the bill. Those concerns are reasonable.
One of the biggest gaps in online information is practical guidance about affordability. As noted by New Era Rehabilitation's discussion of PHP affordability and payer questions, many people aren't just asking whether PHP is clinically helpful. They're asking, "How much will I pay, and what happens if my insurance denies continued days?"
Start with the words on your insurance card
Insurance language sounds more complicated than it is. Here are the terms families usually need first:
- Deductible means the amount you may need to pay before insurance starts covering certain services.
- Copay means a set amount you may owe for a visit or service.
- Coinsurance usually means you and the insurance plan split the cost by percentage, though the exact split depends on your plan.
- Pre-authorization means the insurer may want approval before covering treatment or continued treatment days.
- Out-of-pocket maximum is the point where your plan may begin covering more of the allowed cost, depending on the policy.
You don't need to become an insurance expert overnight. You just need enough clarity to ask the next right question.
What to ask when you call
When you contact your insurer, keep a pen nearby. Ask them to explain the answers in plain language if needed. You can say, "I'm checking behavioral health benefits for partial hospitalization substance use treatment."
Ask about:
- Whether PHP is covered under your behavioral health benefits
- Whether the program must be in-network
- Whether pre-authorization is required before starting care
- What your deductible, copay, or coinsurance would be
- What happens if the insurer stops approving days and the clinical team requests more time
- Whether telehealth PHP is covered, if transportation or work logistics are concerns
Write down the name of the representative, the date, and any reference number for the call. If confusion comes up later, that record helps.
A note for military families and TRICARE users
TRICARE beneficiaries often want to know whether substance use treatment is covered and whether the provider works with military families regularly. That second question matters. Coverage is one piece. Knowing how to handle authorization and documentation is another.
If you're using TRICARE, ask both the insurer and the treatment program how they handle approvals, updates, and changes in level of care. If PHP doesn't fit financially or logistically, ask whether a lower-intensity or telehealth option may be more realistic while still keeping treatment active.
Finding the Right PHP Questions to Ask Providers
Not every program offering PHP will feel the same. Two centers can use the same level-of-care label but deliver very different experiences. One may feel organized, attentive, and clinically strong. Another may feel generic, rushed, or poorly matched to your needs.
A good phone call with a provider should leave you feeling clearer, not more confused. If you feel pressured, brushed off, or given vague answers, pay attention to that.
Questions that reveal how a program actually works
Ask direct questions, even if you feel awkward. You are not being difficult. You are checking whether this is a safe place to trust with recovery.
Who is on the treatment team?
Ask whether the program includes licensed counselors, therapy staff, medical oversight, and support for co-occurring mental health needs.How do you handle psychiatric concerns?
If anxiety, depression, trauma, or mood instability are part of the picture, ask how those issues are treated alongside substance use.What does a typical treatment day look like?
You don't need every minute. You do need a clear sense of group therapy, individual sessions, medication support, and what happens if someone is struggling.How is family involved?
Some people want strong family participation. Others need careful boundaries. The program should be able to explain its approach.What happens if the current level of care isn't enough?
Good providers think in terms of continuity. They should be able to explain what happens if someone needs to step up or step down.
Questions that protect you from surprises
These are the questions people often forget until later:
Transportation and attendance
What happens if a patient misses a day? How does the program support consistent attendance?Insurance communication
Who handles benefit verification, authorization updates, and appeals if coverage becomes complicated?Aftercare planning
Ask how discharge planning works. Recovery doesn't end when PHP ends.
A strong provider should be able to explain treatment in everyday language. If every answer sounds like a brochure, keep asking.
Green flags to listen for
You don't need polished marketing. You need signs of competence and care.
Look for providers who speak specifically about individualized plans, co-occurring support, communication with families when appropriate, and a realistic plan for what comes after PHP. The best answers usually sound calm and concrete. They don't overpromise. They tell you how the program works when things are going well and when they are not.
Your Next Step to Recovery in Northern California
If you're weighing a partial hospitalization program rehab option, you're probably not looking for more jargon. You're looking for a path that makes sense for a real person with a real life. PHP can offer that middle ground. It provides strong clinical structure, daily support, and a practical way to keep recovery moving without requiring full residential living.
For people in Yuba City and across Northern California, local guidance matters. It helps to talk with a team that understands substance use, co-occurring mental health concerns, insurance questions, and the emotional reality families carry into that first call.
Addiction Resource Center LLC offers compassionate addiction care in Yuba City, including help for adults who need structured treatment, support with medication-assisted treatment, and guidance for families trying to understand their options. Their team includes medical and counseling professionals, accepts major insurance plans, and welcomes TRICARE beneficiaries. They are located at 1002 Live Oak Blvd., Suite A, Yuba City, CA, and their 24/7 phone and text line is 530-625-7910.
If you don't know what level of care fits, that's okay. A confidential assessment and insurance verification can help turn a swirl of fear into a practical next step.
If you or someone you love needs help, Addiction Resource Center LLC can walk you through your options with compassion and clarity. Their team can help arrange a confidential assessment, verify insurance benefits, and explain what treatment may fit best, including support for TRICARE families. Call or text 530-625-7910 anytime, day or night, or visit them at 1002 Live Oak Blvd., Suite A, Yuba City, CA to start the conversation.