You may be reading this after another bad night. Maybe sleep has become irregular, your mood swings are sharper, money is disappearing faster than it should, and the promises you made to yourself keep getting pushed to tomorrow. Or maybe you're the family member watching someone you love stay up for long stretches, crash hard, …
You may be reading this after another bad night. Maybe sleep has become irregular, your mood swings are sharper, money is disappearing faster than it should, and the promises you made to yourself keep getting pushed to tomorrow. Or maybe you're the family member watching someone you love stay up for long stretches, crash hard, and insist they can stop anytime.
That moment matters.
People usually don't reach out because life is easy. They reach out because something has started to feel unsustainable. The good news is that stimulant addiction treatment is not guesswork. There is a clear treatment path, and it works best when people understand what kind of help to seek, what questions to ask, and what real recovery looks like when there isn't a medication that replaces the drug.
This guide is built for that practical decision point. It focuses on how stimulant treatment works, how to choose the right level of care, and what to expect once treatment starts.
Table of Contents
- The Moment You Know It's Time for a Change
- Understanding Stimulant Use Disorder and Its Signs
- Evidence-Based Therapies That Actually Work
- Navigating the Different Levels of Treatment Care
- How to Choose the Right Treatment Program for You
- Your Journey Through Treatment and Aftercare
- Take the First Step Today at Addiction Resource Center
The Moment You Know It's Time for a Change
A lot of people know it's time before they say it out loud.
It might happen at work, when concentration turns into agitation and small mistakes start piling up. It might happen at home, when someone notices you've become defensive, secretive, or absent even when you're physically in the room. It might happen after a crash, when the exhaustion, depression, and guilt feel heavier than the temporary lift the stimulant once gave you.
Stimulant problems rarely look dramatic every day. More often, they look inconsistent. A person can still show up, still function in spots, still explain things away. That's part of why stimulant addiction treatment often gets delayed. People compare themselves to a stereotype instead of paying attention to the actual pattern in front of them.
You don't need to wait for a catastrophe to qualify for help. Repeated loss of control is enough reason to act.
I've worked with people who came in after months of saying, "It's not that bad," while their sleep, finances, relationships, and mental health kept getting worse. The turning point was usually simple. They got tired of organizing their life around using, recovering from using, or hiding both.
That recognition is painful, but it's also useful. Once the problem is properly acknowledged, decisions get clearer. You can stop chasing short-term fixes that don't hold and start looking for treatment that matches the underlying issue.
A good treatment process doesn't shame you. It helps you answer practical questions:
- What level of care do I need right now
- What therapies help with stimulant use
- How do I manage work, family, or housing while getting treatment
- What happens after the first few weeks
Recovery starts there. Not with perfect confidence, and not with certainty. It starts when you decide that continuing as-is costs too much.
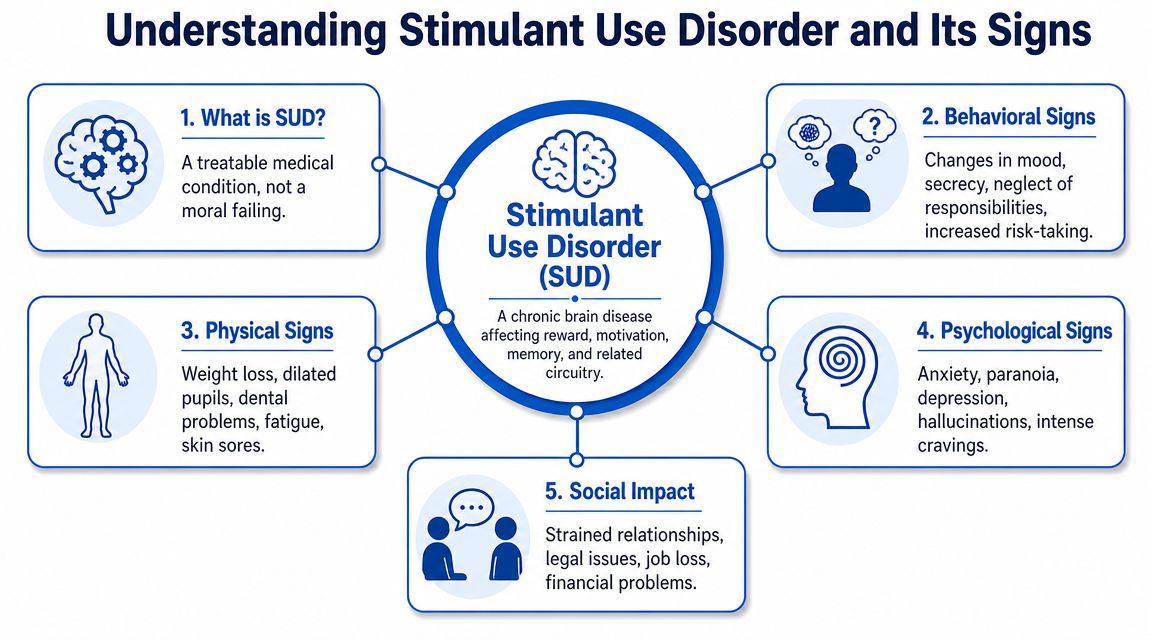
Understanding Stimulant Use Disorder and Its Signs
Stimulant use disorder means stimulant use has moved beyond occasional or controlled use and become compulsive enough to cause harm. That can involve methamphetamine, cocaine, or misuse of prescription stimulants. Clinically, the diagnosis is based on a pattern of impaired control, risky use, craving, and continued use despite consequences.
When use becomes a disorder
In plain language, the line is usually crossed when the drug starts taking priority over judgment.
A person may intend to use a small amount and then keep going. They may spend a lot of time getting stimulants, using them, recovering from them, or trying to manage the fallout. They may keep using after clear problems show up, including conflict at home, mental health instability, legal issues, or physical decline.
In the U.S., an estimated 4.3 million people had a stimulant use disorder in 2024, according to Addiction Policy Forum's summary of SAMHSA data. If this is happening in your life or your family, you're not dealing with something rare.
For readers trying to understand diagnosis language, billing terms, or how substance use conditions are documented in treatment settings, One For All Medical Billing's ICD-10 guide is a useful overview.
Warning signs people often miss
Some warning signs are obvious. Others get mislabeled as stress, burnout, or a "rough phase."
Common warning signs
Behavioral changes include secrecy, lying about whereabouts, impulsive spending, neglecting responsibilities, staying out for long periods, or taking risks that weren't typical before.
Physical changes can include major sleep disruption, appetite loss, weight loss, crashing after periods of being overactivated, skin picking or sores, dental decline, or looking physically depleted.
Psychological signs may show up as anxiety, irritability, paranoia, depression, agitation, intense cravings, or feeling unable to function normally without the drug.
Social fallout often includes strained relationships, work problems, isolation, financial instability, and repeated conflict around trust.
Not every person shows every sign. Some people present as high energy and productive until they don't. Others look depressed, withdrawn, and exhausted between episodes of use. That's why families often miss the pattern at first.
Two things matter clinically. First, stimulant use can create a cycle of overactivation followed by depletion. Second, people often try to solve the crash with more stimulant use, which deepens the pattern. When that loop is established, outside structure usually becomes necessary.
If you're unsure whether this has crossed into disorder territory, look less at isolated incidents and more at the trend. Is life getting narrower, harder to manage, or more chaotic around stimulant use? If the answer is yes, treatment is worth serious consideration.
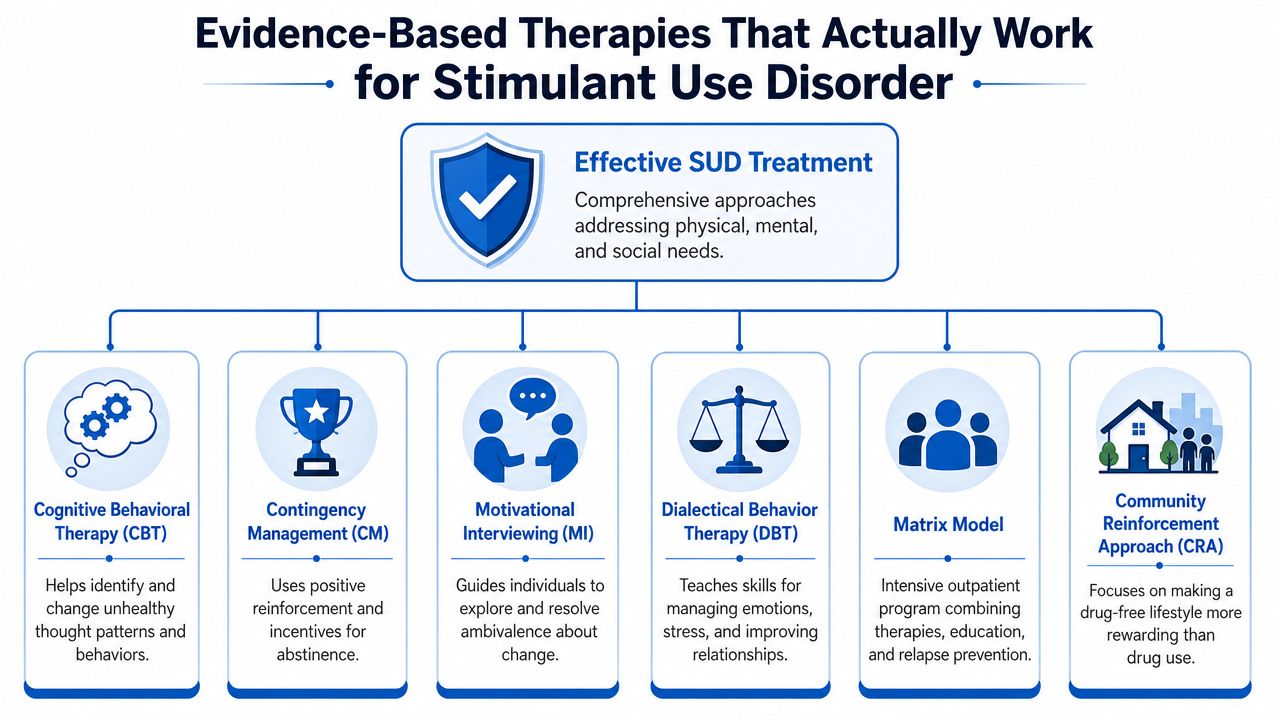
Evidence-Based Therapies That Actually Work
The hard truth about stimulant addiction treatment is that there isn't an FDA-approved medication specifically for stimulant use disorder. That changes the whole treatment model. Instead of a medication-first approach, treatment depends on structured behavioral care that helps people interrupt use, stay engaged, and build a life that can compete with the pull of the drug.
HHS emphasizes that the core of evidence-based stimulant treatment is behavioral therapy, especially contingency management, cognitive behavioral therapy, and motivational interviewing delivered across a continuum of care, as outlined in its review of state and community stimulant treatment efforts.
A visual summary helps clarify the treatment picture.
Why behavioral treatment leads
Stimulants train the brain to chase immediate reward. Effective therapy has to do two jobs at once. It has to reduce the power of that reward loop, and it has to help the person function through cravings, stress, boredom, shame, and everyday triggers without going back to use.
That is why generic advice usually fails. "Just stop." "Stay busy." "Want it more." None of those are treatment plans. People improve when therapy is specific, repetitive, and tied to real behavior.
The strongest lever is often contingency management, or CM. In practice, CM links progress to immediate reinforcement. Instead of waiting for some distant payoff, the patient earns tangible rewards for target behaviors such as attendance, participation, or stimulant-negative testing. Done well, it gives the brain a new reason to choose recovery today, not just eventually.
Later in the treatment process, this explainer gives a concrete example of the time commitment CM usually requires.
Here is a helpful clinical overview before moving on:
What each therapy is doing
CBT works on patterns. Cognitive Behavioral Therapy helps people identify the chain that leads to use. That chain might start with exhaustion, conflict, payday, loneliness, a certain contact, or the belief that stimulants are the only way to get through the day. CBT teaches people to catch the thought, interrupt the routine, and replace it with a practiced response.
Motivational Interviewing works on ambivalence. Many people entering treatment are divided. One part wants relief. Another part still sees stimulant use as useful. Motivational interviewing doesn't argue with the patient. It helps them state, hear, and strengthen their own reasons for change.
Clinical reality: Motivation matters, but structure matters more. Good treatment doesn't wait for perfect readiness before it starts building recovery habits.
Community Reinforcement Approach and related skills-based work change the environment. If the person's daily life still revolves around people, places, and routines tied to stimulant use, therapy has to address that. This means building sober structure, healthier rewards, work and housing stability, and support from people who aren't using.
DBT-informed skills or trauma-informed counseling can help when emotions run hot. Some patients use stimulants around trauma, panic, anger, or emotional numbness. In those cases, treatment needs to teach distress tolerance, emotion regulation, and safer ways to handle overwhelm.
What doesn't work well is treatment that stays vague. A person struggling with stimulants needs a plan that tracks behavior, responds quickly to setbacks, and keeps care moving forward.
Navigating the Different Levels of Treatment Care
People often assume treatment is one place. It isn't. It's a continuum. The better way to think about stimulant addiction treatment is as a set of stair steps. You start at the level that matches your current risk, stability, and support, then step down as you get stronger.
Think in stair steps, not all or nothing
Some people need high structure immediately. Others are stable enough to begin in outpatient care. The right starting point depends on the full picture, including current use, mental health symptoms, home environment, medical needs, relapse risk, and whether the person can safely function outside a treatment setting.
Across substance use treatment in 2024, many people entered care through different doors, including outpatient, telehealth, and inpatient settings, which shows why a full continuum matters. That pattern is described in the treatment access breakdown summarized earlier from national data.
A few practical distinctions help:
- Detox or withdrawal management is about stabilization. For stimulant users, this often means managing the crash period, exhaustion, agitation, depression, sleep disruption, and safety concerns rather than treating a classic alcohol or opioid withdrawal syndrome.
- Residential treatment is about immersion. It removes the person from immediate access, creates daily structure, and gives staff more opportunities to intervene when cravings, impulsivity, or psychiatric symptoms rise.
- Intensive Outpatient Programs are for people who need frequent treatment but can live at home or in supportive housing.
- Standard outpatient and telehealth care fit people who are more stable, stepping down from a higher level, or balancing recovery with work, childcare, or transportation limits.
The best level of care is the one the patient can engage in consistently and safely, not the one that sounds most impressive.
How the levels compare
| Level of Care | Primary Goal | Time Commitment | Best For |
|---|---|---|---|
| Detox or withdrawal support | Stabilize sleep, mood, safety, and immediate functioning | Short-term and intensive | People coming off a binge, crashing hard, or struggling with acute psychiatric or physical instability |
| Residential rehab | Create full structure and separation from using environments | Daily live-in care | People with repeated relapse, unsafe housing, heavy environmental triggers, or poor treatment follow-through |
| Intensive Outpatient Program | Deliver frequent therapy while maintaining community life | Several treatment contacts each week | People who need more than weekly counseling but don't require live-in care |
| Outpatient counseling | Build skills, monitor progress, and support longer-term recovery | Flexible and ongoing | People with stronger stability, step-down needs, or mild to moderate impairment |
| Telehealth treatment | Maintain access and continuity when in-person care is hard | Flexible remote sessions | People with work demands, transportation barriers, family obligations, or rural access issues |
Some providers can connect these steps more smoothly than others. For example, Addiction Resource Center LLC offers medically supervised detox, partners for residential rehabilitation through Ona Treatment Center, and provides in-person and telehealth IOP, which is the kind of continuum many patients need when recovery doesn't happen in a straight line.
The trade-off is straightforward. More structure gives more protection, but less flexibility. More flexibility helps people stay connected to normal life, but it also exposes them to triggers sooner. Good treatment planning balances both.
How to Choose the Right Treatment Program for You
Choosing a program shouldn't come down to the nicest website or the fastest admissions call. The quality of stimulant addiction treatment depends on fit. If the program can't handle your actual life, it won't matter how polished the marketing sounds.
Modern guidance emphasizes that treatment should be customizable enough to address co-occurring depression or anxiety, housing instability, and flexible access such as telehealth, as described in Learn About Treatment's overview of care for stimulant use disorder.
Questions worth asking before you commit
Start with direct questions. You are not being difficult. You are checking whether the program understands stimulant treatment beyond generic rehab language.
- How do you treat stimulant use specifically Ask whether the program uses contingency management, CBT, motivational interviewing, and structured relapse prevention rather than relying on vague counseling alone.
- How do you assess mental health Anxiety, depression, trauma symptoms, paranoia, and sleep disruption often shape stimulant use. If a program treats those as side issues, that is a problem.
- What happens if I relapse or miss sessions Good programs have a plan for setbacks. They don't respond with confusion or immediate discharge unless safety requires it.
- Can you offer telehealth or schedule flexibility This matters for people with jobs, childcare, transportation barriers, or inconsistent housing.
- What does step-down planning look like You want to know how the provider handles movement from detox to residential, from residential to IOP, or from IOP to outpatient support.
- Do you accept my insurance Ask this early. If you're a veteran or military family member, ask specifically about TRICARE.
What a solid program should be able to handle
A strong program should be comfortable with complexity. Stimulant use rarely appears in a tidy package. Someone may also be dealing with panic, trauma, relationship conflict, legal stress, unstable work, or a living situation where other people are still using.
Look for signs that the provider thinks in systems, not slogans:
Practical rule: If a program only talks about detox, discipline, or "wanting sobriety enough," keep looking.
You also want clarity about staffing and scope. Who is doing the assessment? Is there access to medical care if symptoms worsen? Are there licensed counselors involved? Is family support available when appropriate? Does the provider understand that stimulant recovery often requires accountability plus flexibility, not one or the other?
Another good sign is honesty about trade-offs. Residential care can offer protection and structure, but not everyone can leave work or home responsibilities. Telehealth can widen access, but it won't be enough for a patient who is actively psychotic, severely unstable, or unable to stop using without a controlled setting. The right program says that plainly.
Finally, pay attention to how the first conversation feels. You should leave with more clarity than you had before. Not pressure. Not confusion. Not a sales pitch.
Your Journey Through Treatment and Aftercare
Treatment works better when people know what to expect. Most anxiety around care comes from the unknown, not the actual process.
What treatment usually looks like day to day
The first step is usually an assessment. Staff will ask about your stimulant use, other substances, mental health symptoms, sleep, medical concerns, safety, family situation, and prior treatment. This isn't about catching you in contradictions. It's about building a plan that fits.
After that, treatment usually includes a mix of individual counseling, group therapy, structured skill-building, and recovery planning. The content often focuses on triggers, cravings, routines, thought patterns, relationships, emotional regulation, and what to do in the hours when people are most likely to return to use.
For stimulant treatment, sustained engagement matters. Pew notes that contingency management is typically delivered for a minimum of 12 weeks with urine testing two to three times per week, which shows how recovery is built through repeated participation rather than a single event, as described in Pew's stimulant treatment fact sheet.
That timeline matters because people often expect to feel "fixed" quickly. The early phase is usually less about confidence and more about repetition. Show up. Follow the plan. Let structure carry you while your judgment and stability improve.
Aftercare is where stability gets built
A lot of people think aftercare is optional. It isn't. Once formal treatment intensity drops, daily life returns with all the old triggers attached. If there is no plan for that shift, risk rises.
Strong aftercare usually includes several pieces working together:
- Step-down treatment such as moving from residential to IOP, or from IOP to outpatient counseling.
- Ongoing accountability through therapy, check-ins, drug testing when clinically appropriate, and continued recovery goals.
- Support network building through family work, peer support, recovery meetings, sober housing, or trusted non-using relationships.
- Relapse prevention planning that names the highest-risk people, places, thoughts, and times of day.
Recovery is usually less about one big breakthrough and more about many small decisions made with support.
Relapse prevention isn't about proving willpower. It's about reducing exposure, increasing structure, and recognizing warning signs early. People do better when they know what their risk pattern looks like and have a written response before a crisis starts.
Take the First Step Today at Addiction Resource Center
By the time individuals search for stimulant addiction treatment, they've already spent a lot of energy trying to manage it alone. They've cut back and restarted. They've hidden it, justified it, or promised themselves this was the last time. At some point, the better use of energy is getting assessed and finding out what level of care fits.
The path doesn't have to be complicated. You need a starting point, a clear recommendation, and a plan that accounts for the realities of your life. That means looking at substance use, mental health, schedule, relapse risk, housing, transportation, family responsibilities, and what kind of support you'll need after the first phase of treatment.
Addiction Resource Center in Yuba City is built around that kind of practical care. It offers medically supervised detox, access to residential rehabilitation through its partner facility, in-person and telehealth IOP, treatment for co-occurring mental health needs, and support from a multidisciplinary team that includes medical, counseling, and recovery staff. It also accepts most major insurance plans and welcomes TRICARE beneficiaries.

If you're not sure what you need, that's okay. A good first call isn't a commitment to one program. It's a way to get oriented. The immediate questions are simple:
- Are you safe right now
- Do you need detox, residential support, or outpatient care
- Are mental health symptoms making the situation more urgent
- Can treatment be arranged around work, family, or transportation
- What will insurance cover
If you're asking these questions for a loved one, the same principle applies. You do not need to solve the whole situation before contacting a provider. You need the next clinical step.
Waiting for more certainty usually just gives the disorder more time. A conversation with a treatment team can replace guesswork with a real plan.
If you or someone you love needs help, contact Addiction Resource Center LLC to talk through options confidentially. You can call or text their 24/7 line at 530-625-7910, ask about insurance verification, or schedule a consultation to find out whether detox, residential care, in-person IOP, or telehealth treatment makes the most sense.