You may be sitting at your kitchen table with ten browser tabs open, trying to decide what could keep your spouse, son, daughter, or yourself alive and stable. One center says inpatient. Another says outpatient. A third says detox first. Everyone sounds confident, and you're the one left carrying the fear. I want to simplify …
You may be sitting at your kitchen table with ten browser tabs open, trying to decide what could keep your spouse, son, daughter, or yourself alive and stable. One center says inpatient. Another says outpatient. A third says detox first. Everyone sounds confident, and you're the one left carrying the fear.
I want to simplify this for you.
The question usually isn't “Which rehab is better?” The pertinent question is, what level of care gives this person the best chance to start recovery safely and stay in it long enough for it to take hold? Sometimes that means living in a facility. Sometimes it means getting structured care while staying at home. Very often, it means both, in sequence.
If you're trying to make this decision under pressure, start here: choose the setting that matches the person's current risk, home environment, and ability to follow through. Convenience matters, but safety matters more.
Table of Contents
- Making the Most Important Decision
- Defining the Two Paths to Recovery
- Inpatient vs Outpatient A Side-by-Side Comparison
- Who Is the Best Fit for Inpatient Rehab
- When Is Outpatient Rehab the Right Choice
- Beyond a Single Choice The Continuum of Care
- Your Next Step to Recovery in Northern California
Making the Most Important Decision
Families often come to this choice exhausted. They've already lived through missed work, mood swings, broken promises, panic after a binge, or the slow dread of watching someone disappear into alcohol or drugs. By the time they ask about inpatient vs outpatient rehab, they're not asking an academic question. They want to know what will work.
That urgency is appropriate.
If someone is medically unstable, emotionally falling apart, living in chaos, or relapsing every time they try to quit at home, I'll be direct. Don't choose the least disruptive option. Choose the safest one. Too many families lose time by trying to force outpatient care on a situation that clearly needs a protected setting.
The best rehab plan is the one the person can enter safely, complete, and continue after discharge.
At the same time, not every person needs to leave home for treatment. Some people have a steady place to live, reliable support, and enough internal readiness to attend care consistently while staying connected to work, family, or school. For them, outpatient can be the right call.
What families usually get wrong
The biggest mistake is treating this as a one-time fork in the road. It rarely is. A person may need detox first, then residential treatment, then a step-down program. Another person may start in an intensive outpatient track and move up if they can't stay sober.
A second mistake is choosing based on image. Inpatient isn't “better” because it sounds more serious. Outpatient isn't “weaker” because it sounds more flexible. The right fit depends on what the person can safely manage today.
The standard I use
Ask three questions first:
- Can they stay safe outside a facility?
- Will their home environment support recovery or sabotage it?
- Can they reliably show up and participate without 24-hour structure?
If the answer to those questions is shaky, I lean toward a higher level of care.
Defining the Two Paths to Recovery
A family often reaches this point after a hard week. Someone has agreed to get help, but now everyone is asking the same question. Do they need to leave home, or can they start treatment while staying in their daily life?
Here is the clearest way to define the difference. Inpatient treatment means living at the rehab facility full time. Outpatient treatment means living at home and showing up for treatment on a set schedule. That distinction matters, but it is only the starting point. Good treatment planning looks at where the person starts and what level of care should come next.
One treatment overview notes that inpatient rehab commonly lasts about 28 days or longer, while outpatient care lets the person remain at home and attend scheduled services, as outlined by this overview of inpatient and outpatient treatment levels.
What inpatient rehab actually means
Inpatient rehab is usually called residential treatment. The person sleeps there, eats there, attends therapy there, and spends the day inside a setting built around recovery. That distance from home is not a formality. It changes the rhythm of the day, lowers exposure to triggers, and gives staff more chances to intervene before a bad hour becomes a bad decision.
I recommend families view inpatient as a stabilization setting, not a final destination. For many people, it is the first protected step in a longer recovery plan that later includes outpatient care and aftercare support.
Outpatient includes several levels of care
Outpatient is not one thin layer of treatment. It ranges from near-daily clinical programming to standard weekly visits, and that range is why outpatient can work very well for the right person.
The same source describes a few common levels:
- Partial Hospitalization Program (PHP) offers treatment for several hours a day, most days of the week.
- Intensive Outpatient Program (IOP) provides a lower but still structured number of treatment hours across the week.
- Standard outpatient care is lighter and usually works best for people who are more stable or stepping down from a higher level of care.
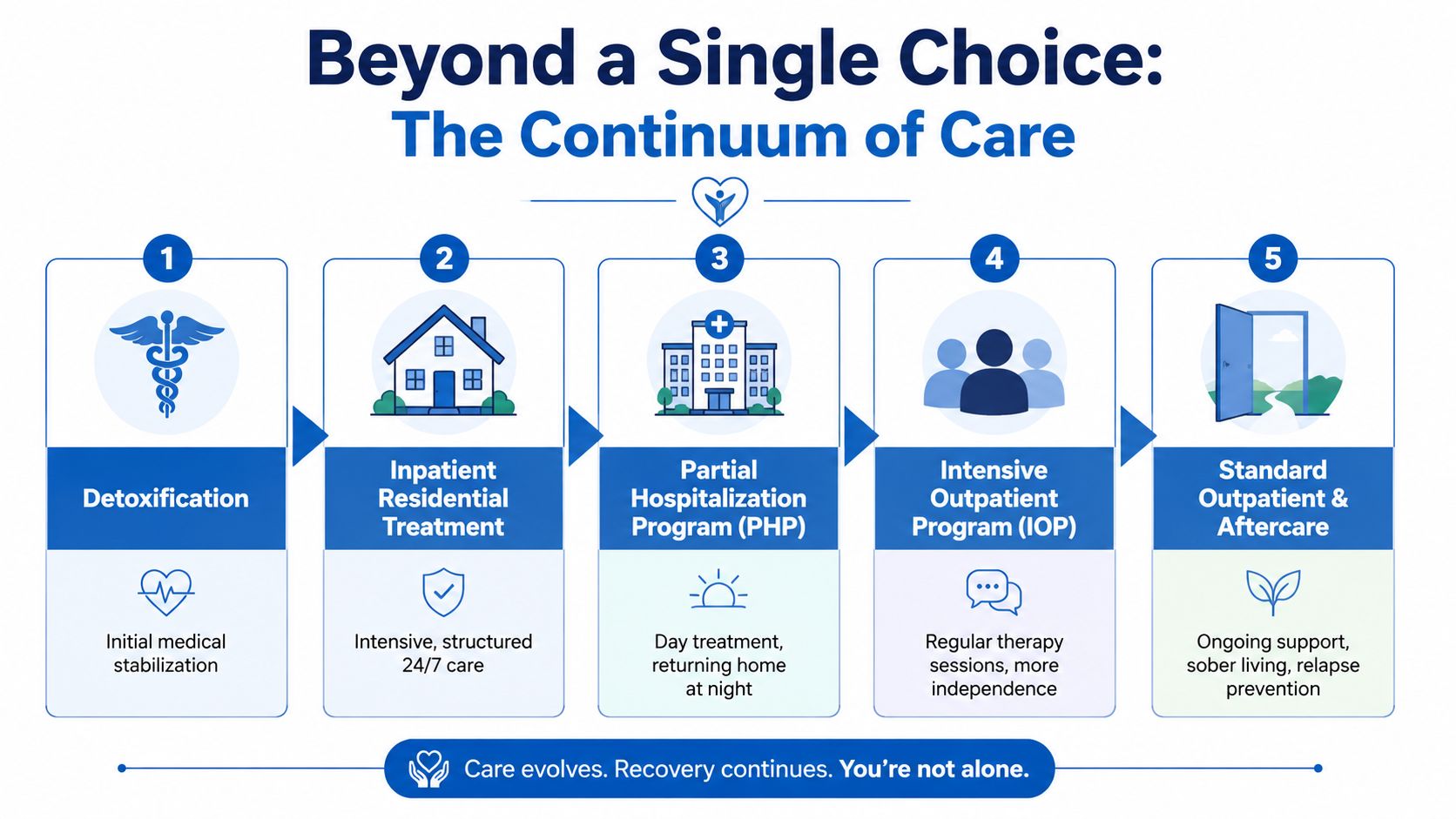
That progression matters. A person may start in residential treatment, step down to PHP, continue in IOP, and then stay connected through outpatient counseling and recovery support. That is how treatment works in real life. It is a continuum of care, not a single yes-or-no choice.
Why the setting changes the recovery experience
The setting shapes what recovery asks of the person each day. Inpatient care reduces outside distractions and gives constant structure. Outpatient care asks the person to practice recovery while still dealing with work stress, family conflict, access to substances, and the habits tied to using.
Transitions between those levels deserve real attention. This challenge is not unique to addiction care. Many healthcare providers focus on streamlining medical practice workflows so patients do not get lost between appointments, referrals, and follow-up. In addiction treatment, a missed handoff can mean relapse, overdose, or dropping out of care entirely.
That is why families should stop asking which option sounds better and start asking which level of care the person can safely start now, and where they should step next once they are stable enough to keep going.
Inpatient vs Outpatient A Side-by-Side Comparison
A family calls after another frightening weekend. They want a simple answer. Should he go away to treatment, or stay home and attend sessions nearby?
My answer is direct. Start by matching the level of care to the level of risk, then plan what comes next. Inpatient and outpatient are not competing philosophies. They are different points on the same recovery path.
Here's the quick view.
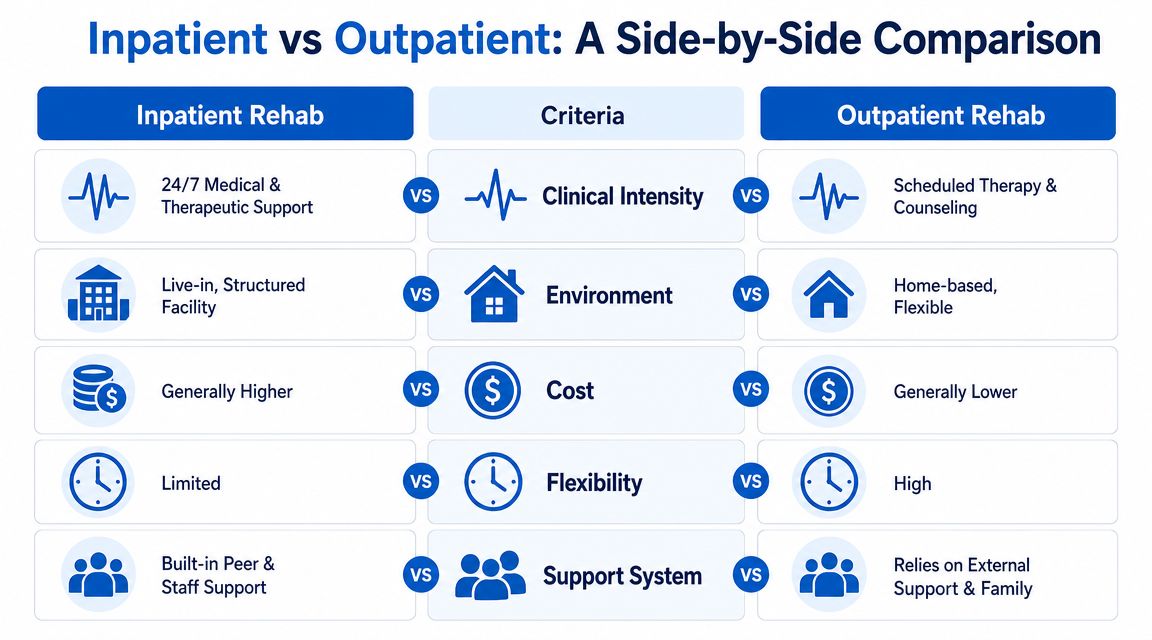
| Criterion | Inpatient (Residential) Rehab | Outpatient Rehab |
|---|---|---|
| Living arrangement | Lives at the treatment facility | Lives at home |
| Structure | Highly structured daily routine | Scheduled sessions with more independence |
| Supervision | Continuous on-site support | Intermittent clinical contact |
| Exposure to triggers | Reduced during treatment | Ongoing exposure to real-world triggers |
| Flexibility | Limited | High |
| Fit | Higher-acuity situations, unstable environment, repeated relapse | Stable environment, reliable support, manageable daily risk |
Cost and completion are the central trade-off
One evidence summary in the NCBI Bookshelf reports that outpatient rehab averages about $5,000 for three months, compared with about $10,000 for one month of residential care and $12,500 for one month of inpatient care with detox, as described in this NCBI review of treatment settings and costs.
That cost gap matters to families. So does treatment completion. Those are related, but they are not the same question, and they should not be treated as if they come from the same source.
Here is the practical takeaway. Outpatient is often easier to reach financially and logistically. Inpatient often gives a struggling person enough structure to stay engaged through the hardest early stretch of recovery.
Core trade-off: Inpatient creates more disruption at the start. Outpatient requires the person to manage more exposure and more temptation while still medically and emotionally fragile.
Environment changes what recovery asks of the person
In inpatient care, the setting removes many of the decisions that fuel relapse. The person is not going home to the same argument, the same dealer, the same bottle in the cabinet, or the same lonely routine night after night.
Outpatient asks for a different kind of strength. The person has to attend treatment and practice recovery while still living inside the life that supported their substance use. For someone with a stable home, good support, and manageable symptoms, that can work very well. For someone with chaos all around them, it often fails for predictable reasons.
Families usually sense this before they can explain it. They know whether home feels like a place to heal or a place to unravel.
Here's a helpful explainer if you're also thinking about how care settings affect communication and follow-through in general medical systems: improving patient experience in medical offices. In addiction treatment, clear scheduling, responsive staff, and consistent follow-up are part of care. They help people stay connected long enough to improve.
What to weigh before choosing
- Medical stability: Active withdrawal, medication complications, or severe psychiatric symptoms push the decision toward inpatient care.
- Recovery environment: A sober, calm home can support outpatient treatment. A home with conflict, instability, or substance use usually cannot.
- Daily responsibilities: Work, school, parenting, and caregiving can make outpatient more realistic, but only if it is also clinically safe.
- Readiness for independence: Some people can use structure without constant supervision. Others need a setting that holds the day together for them.
- Next step after stabilization: The best programs do not stop at admission. They map out what follows, whether that means stepping down from detox to residential, from residential to IOP, or from outpatient to long-term aftercare.
This short video may help if you're sorting through the practical differences:
Who Is the Best Fit for Inpatient Rehab
Some people need a stronger container. That's what inpatient rehab is for.
If the person you're worried about has high daily substance use, repeated relapse, severe cravings, unstable housing, serious emotional volatility, or a home environment that keeps dragging them back into use, I would not start with the lightest option available. Residential treatment exists because some people cannot stabilize while sleeping in the same bed, seeing the same people, and facing the same triggers every night.
The strongest candidates for inpatient care
I push families toward inpatient when several of these are true:
- Home isn't safe for recovery: Other people are using, there's constant conflict, or the person doesn't have stable housing.
- Past treatment didn't hold: They've tried counseling, meetings, or outpatient care and kept dropping out or relapsing.
- Their functioning is falling apart: They can't keep routines, follow through, or regulate themselves long enough to benefit from a lower level of care.
- They need containment: Not punishment. Containment. They need a place where recovery is the default setting for the day.
Why I lean this way in high-risk cases
A large U.S. treatment dataset found that residential and inpatient care outperformed outpatient care on treatment completion. In that dataset, outpatient accounted for 84.6% of episodes and had a 51.9% completion rate, while residential treatment had a 64.5% completion rate. After adjusting for client, clinical, and state-level differences, residential clients were still reported as more than three times as likely to complete treatment as outpatient clients, according to this analysis of residential versus outpatient treatment completion.
That matters most for people who already have engagement risk. If someone is unstable, ambivalent, homeless, cycling through crises, or constantly derailed by their environment, completion is not a side issue. It's one of the biggest predictors that treatment will have a chance to work.
If a person keeps failing in an unstructured setting, the answer usually isn't less treatment. It's more support and more structure.
What families should stop doing
Stop asking whether inpatient seems “too extreme.” Ask whether the current situation is already extreme.
If the person can't string together even a few sober days at home, isn't showing up consistently, or falls apart the minute pressure hits, then inpatient isn't overreacting. It's matching the level of care to the level of risk.
When Is Outpatient Rehab the Right Choice
Outpatient rehab is the right choice when the person has enough stability to use treatment, not just attend it. That distinction matters. A person can sit in a group and still be set up to fail if everything outside that building is working against them.
The best outpatient candidates usually have a decent place to live, at least one reliable support person, and the ability to stay accountable between sessions. They don't need 24-hour structure to remain engaged. They need skilled treatment that fits real life.
Signs outpatient can work well
Outpatient often makes sense when the person:
- Has a stable home base: Not perfect, just predictable and reasonably safe.
- Can manage daily responsibilities: Work, school, parenting, or caregiving still matter, and stepping away completely may do more harm than good.
- Will show up consistently: Motivation doesn't have to be flawless, but it does need to be real.
- Can tolerate real-world exposure: They're able to practice coping skills while still living in the environment where recovery has to happen.
A real advantage outpatient has
A clinically important distinction between settings is the kind of monitoring each one supports. Inpatient care is built for rapid stabilization and frequent supervision. Outpatient care is better suited to ongoing symptom and functional tracking over time, which allows clinicians to adjust the treatment plan as the person goes about daily life, according to this discussion of rehab outcome measures and monitoring cadence.
That's one reason I respect good outpatient programs. They don't just provide flexibility. They let clinicians see what happens when the person goes home, returns to work, argues with a partner, passes old triggers, and still has to make decisions.
Practical rule: Outpatient is a good fit when the outside world is challenging but not actively defeating recovery every day.
What outpatient is not
It is not a consolation prize. It is not “rehab lite.” A well-run outpatient program can be demanding, clinically serious, and highly effective for the right person.
It also requires honesty. If the person says they can stay sober at home and every recent week says otherwise, the treatment plan needs to change. Good outpatient care works because it adjusts. It shouldn't pretend stability exists when it doesn't.
Beyond a Single Choice The Continuum of Care
A family gets through detox, breathes for the first time in weeks, and asks the wrong question: “So are we done?” No. Early progress is not the finish line. Recovery holds when the next level of care is already in place before the first one ends.
That is the essential value of a continuum of care. It connects each stage of treatment so the person is not starting over every time their needs change. Someone may begin with detox, move into residential treatment, step down to PHP or IOP, and continue with outpatient therapy and aftercare. Someone else may start in outpatient care, then move up to a higher level if home stops being a safe place to recover.
Why this model matches real recovery
People do not recover in a straight line. A stable week can turn into a dangerous weekend. A strong discharge plan can fall apart once work stress, family conflict, cravings, or depression return.
Good treatment plans expect that. They build in follow-up, step-down care, and room to adjust. That is how you protect progress.
This matters most after a higher level of care. Many people do well in a structured setting because the structure is doing part of the work. Once they go home, every trigger comes back at once. Step-down care keeps clinical support in place while the person relearns daily life sober.
Where telehealth and hybrid care fit
Telehealth and hybrid services belong in that chain of care because they remove practical barriers that often break momentum. If a person cannot get across town three evenings a week, cannot leave work early, or has no childcare, treatment attendance drops fast. A virtual IOP or a hybrid schedule can keep the person engaged instead of losing them during a difficult transition.
That is not about convenience. It is about continuity.
Families should ask a simple question: “What is the plan after this level ends?” If the answer is vague, the plan is weak. A strong provider should be able to explain the next step, the warning signs that call for more support, and how the handoff will happen.
The same principle shows up across healthcare. If you have looked at patient communication systems or a digital front door for practices, you have seen how access, follow-up, reminders, and handoffs affect outcomes. Addiction treatment is no different. Clear transitions keep recovery moving. Poor transitions leave people exposed right when they are most vulnerable.
A better question than “inpatient or outpatient?” is this:
- What level of care is safest right now?
- What support should follow immediately after it?
- What will we do if the first plan stops working?
That is how families make a smart decision. They stop treating rehab as a single choice and start building a path that can hold up in real life.
Your Next Step to Recovery in Northern California
If you're still unsure where your loved one belongs, use a simple checklist. Be honest. Wishful thinking won't protect anyone.
A quick decision checklist
- Choose a higher level of care if the person can't stay sober at home, keeps relapsing, has unstable housing, or falls apart without constant structure.
- Choose outpatient if the person has a stable place to live, can participate reliably, and has enough support to handle life between sessions.
- Choose a continuum plan if the person needs one level now and a different level next. That's common. It's often the smartest route.
- Choose an assessment immediately if your family is stuck in debate and no one can tell what's clinically safe.
The right first step is usually a professional evaluation, not another week of arguing at home.
What to look for in a local program
In Northern California, I'd tell families to look for a provider that can do more than one thing well. You want access to medically supervised detox, a path into residential rehab when needed, and a strong IOP option, including telehealth when logistics get hard. You also want a team that can address both substance use and mental health at the same time, because those problems often travel together.
Look for practical details too:
- Insurance access: Ask whether the program accepts major insurance and whether it welcomes TRICARE.
- Team depth: A medical doctor, nurse, licensed counselors, therapist, and recovery mentors create a stronger safety net than a thin staffing model.
- Aftercare planning: Don't settle for a discharge date without a next-step plan.
If you're in Yuba City or nearby communities, make the next step concrete. Write down the address. Save the number. Ask for a confidential assessment. A real plan is easier to start than a vague intention.
For local families, that means knowing there's a treatment option at 1002 Live Oak Blvd., Suite A, Yuba City, CA, with a 24/7 phone and text line at 530-625-7910. When a person is finally ready, easy access matters.
If you're looking for compassionate, local help, Addiction Resource Center LLC offers a full continuum of care for adults in Yuba City and Northern California, including medically supervised detox with MAT, residential treatment through Ona Treatment Center, and flexible IOP in person or via telehealth. Their multidisciplinary team provides confidential, down-to-earth support for substance use and co-occurring mental health needs, and they welcome most major insurance plans, including TRICARE. Call or text 530-625-7910 any time to request a confidential assessment or ask what level of care fits your situation.