It's late. Someone is locked in the bathroom, passed out on the couch, shaking on the bed, or saying things that make your stomach drop. You may be trying to figure out whether this is a bad night, a relapse, a panic spiral, or a real medical emergency. Treat the next 72 hours as a …
It's late. Someone is locked in the bathroom, passed out on the couch, shaking on the bed, or saying things that make your stomach drop. You may be trying to figure out whether this is a bad night, a relapse, a panic spiral, or a real medical emergency.
Treat the next 72 hours as a bridge, not a single decision. First you keep the person alive. Then you get the right level of care. Then you make sure the handoff happens. That middle ground is where many families get stuck. They know when to panic, and they know rehab exists, but they don't know what to do between those two points.
Emergency addiction treatment lives in that gap. It's practical, immediate, and often messy. The job is not to solve the whole addiction tonight. The job is to make the next safe move, then the next one after that.
Table of Contents
- Recognizing an Addiction Emergency
- Your First Actions in a Crisis
- How to Find and Access 24/7 Emergency Treatment
- The First 24 Hours What to Expect During Admission and Detox
- Navigating Logistics Insurance, Tricare, and Privacy
- From Stabilization to Long-Term Recovery
Recognizing an Addiction Emergency
A lot of people freeze because they're asking the wrong first question. They ask, “Is this really that serious?” A better question is, “Do we need emergency addiction treatment right now, or can this wait until morning?”
Public guidance often leaves people to guess. Health systems such as NYC Health + Hospitals make an important distinction. Some withdrawal can be handled in outpatient settings, but severe symptoms, overdose risk, or psychiatric crisis need immediate higher-level care according to NYC Health + Hospitals addiction services guidance.

What makes this an emergency
An addiction emergency usually falls into one of three lanes:
- Overdose or suspected overdose. Breathing is slow, stopped, or irregular. The person won't wake up. Skin may look pale, gray, or blue.
- Severe withdrawal. This is common with alcohol and can also happen with other substances in ways that become medically dangerous fast. The person may be confused, agitated, vomiting, shaking severely, hallucinating, or having a seizure.
- Substance use plus acute psychiatric danger. Suicidal statements, violent behavior, extreme paranoia, or complete disorientation change the response immediately.
Practical rule: If you're debating whether it's “bad enough,” treat reduced consciousness, breathing changes, seizures, chest pain, or suicidal behavior as emergency-level problems.
Signs that need immediate action
Use this as a quick triage list.
Possible opioid or fentanyl overdose
- Person is hard to wake or unresponsive
- Breathing is very slow, shallow, noisy, or absent
- Lips or fingertips look blue, gray, or pale
- Body is limp
- Pupils look very small
Severe alcohol or sedative withdrawal
- Seizure activity
- Hallucinations
- Severe confusion or disorientation
- Uncontrolled shaking
- Repeated vomiting with inability to keep fluids down
Mental health crisis with substance use
- Talking about wanting to die
- Talking as if others would be better off without them
- Looking for pills, weapons, or other means
- Extreme agitation, panic, or psychosis
- Threatening self-harm or harm to others
Medical red flags
- Chest pain
- Head injury
- High fever
- Trouble walking or repeated falls
- Pregnancy plus withdrawal, overdose risk, or heavy intoxication
This isn't rare background noise in the system. Substance use-related emergency department visits in the United States rose from 2.926 million to 4.132 million between 2013 and 2018, and their share of all ED visits rose from 2.93% to 4.25%, a 45% relative increase, while overall ED volume stayed stable according to a national emergency department study on substance use visits. The practical meaning is simple. Emergency rooms are seeing more addiction crises because more crises are reaching a medical breaking point.
If the person has severe symptoms, stop debating motives, promises, or whether they “meant to” use that much. Triage first. Meaning can wait.
Your First Actions in a Crisis
It is 2 AM. Someone is slumped on the bathroom floor, or pacing and saying they do not want to live, or shaking so hard they cannot hold a cup of water. Family members are talking over each other. One person is crying. Another is trying to get answers. This is the part where minutes get wasted.
Use the next 10 minutes well. The goal in this window is simple: keep the person alive, reduce immediate danger, and get the right level of help in motion. If your mind is blank, put one person in charge and use a written checklist. A caregiving tool like this confident emergency management guide can help one person assign tasks while everyone else follows them.

Start with scene control.
Turn on the lights. Clear the floor around the person. Put pets in another room. Stop anyone from arguing, filming, or trying to force a confession. Open the front door if EMS is coming. Put one phone on speaker. Put one sober adult in charge of the person, and another in charge of gathering what responders will ask for: medication bottles, substances or packaging, ID, insurance card, allergies, and a phone charger.
If you suspect an overdose
Treat an overdose like an overdose before you have proof. Waiting for certainty is how people lose breathing support, lose pulse, or aspirate.
- Call 911.
- Give naloxone if you have it. Follow the package directions.
- Try to wake them. Say their name loudly. Rub your knuckles firmly on the breastbone if needed.
- Support breathing and keep the airway open.
- Place them on their side if they are breathing on their own and may vomit.
- Stay until EMS arrives, even if they wake up.
Give paramedics the shortest useful report you can:
- what they may have used
- when you think they last used
- whether alcohol, pills, fentanyl, or more than one substance may be involved
- whether naloxone was given, and how many doses
- any seizure, fall, head strike, pregnancy, or other medical issue
Use plain language. “He took two blue pills about 20 minutes ago and then stopped responding” is better than a long apology or a guess-filled story.
If the person wakes up angry, sick, or confused, keep going with the plan. Naloxone can wear off while the opioid is still active. A person who wakes up still needs medical evaluation and observation.
If suicide risk is part of the crisis
Substances lower inhibition and raise impulsivity. That means a person can move from talking to acting fast.
Stay with them. Remove immediate means if you can do it safely, including pills, firearms, sharp objects, cords, and car keys. Keep your voice low and your sentences short. Ask directly, “Are you thinking about killing yourself?” Clear questions are safer than vague ones.
Call 911 if there is an attempt, a specific plan with access to means, severe intoxication plus suicidal behavior, psychosis, or you cannot keep the scene safe.
A useful script:
“I'm here. I'm staying with you. Help is on the way.”
Avoid speeches, threats, and debates about treatment. This is not the hour to argue about trust, relapse, or broken promises.
What to do while help is coming
These small actions matter because they shorten the handoff and reduce mistakes.
- Watch breathing and responsiveness. If they stop breathing normally, tell 911 and follow instructions.
- Do not give more substances to steady them. More alcohol, benzodiazepines, or opioids can make the crisis worse.
- Do not force food, coffee, or a shower. None of that fixes overdose, withdrawal, or suicidal risk.
- Keep the environment quiet. Fewer people, fewer questions, less stimulation.
- Write down times. Last known well, last use, naloxone dose, seizure, vomiting, or collapse.
- Secure children and other vulnerable people. They should not be in the middle of the scene.
If you are the sober person in the room, your job is coordination. Speak slowly. Give one instruction at a time. In the first 72 hours, good outcomes often depend less on perfect decisions than on avoiding the obvious bad ones: delay, denial, and disorganized handoffs.
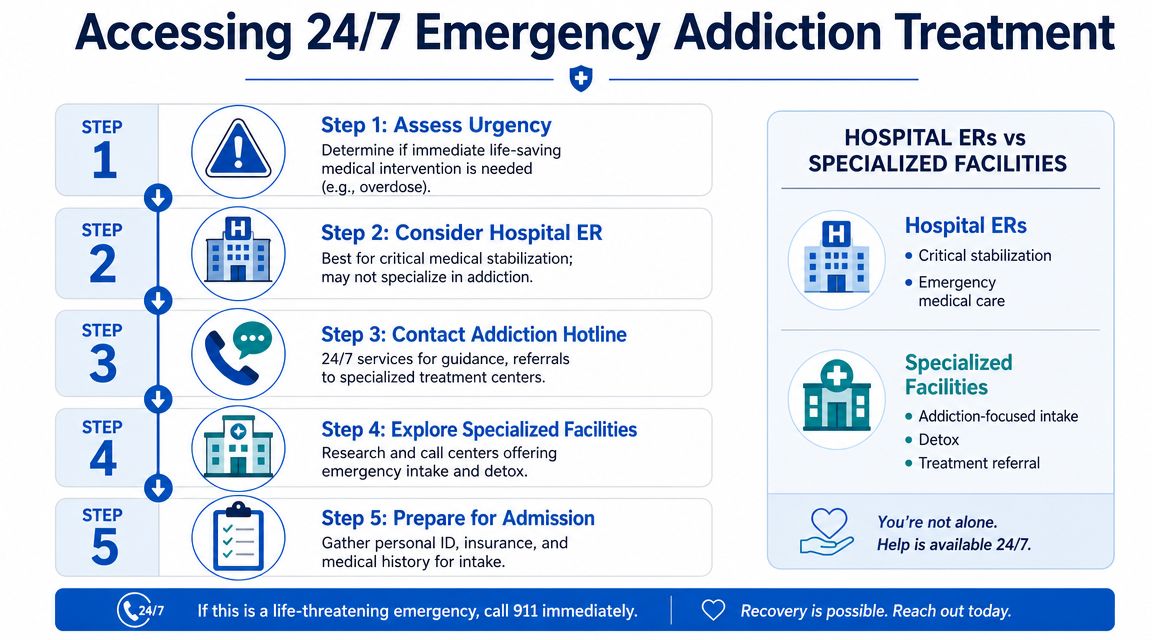
How to Find and Access 24/7 Emergency Treatment
It is 2:13 a.m. The overdose scare has passed, or the person is awake but shaky, panicked, and starting to crash. Everyone in the room wants one answer: where do we go now?
This is the part families often underestimate. The emergency is still active, even if the person is breathing and talking. In the first 72 hours, the primary job is to get from crisis to the right level of care without losing time in a bad handoff, a long wait, or a facility that cannot manage the medical risk.
When to call 911 and when to call a facility
Use the person's current condition, not their promises, to make the call.
| Situation | Best first move |
|---|---|
| Not breathing, barely breathing, seizure, severe confusion, overdose, suicidal danger, chest pain | Call 911 |
| Awake, medically stable, needs detox, escalating withdrawal, recent relapse without immediate life threat | Call a treatment facility admissions line |
| Unsure whether symptoms are severe withdrawal or medical crisis | Call 911 |
An ER is built for immediate medical stabilization. A detox or addiction treatment program is built for withdrawal management, medication evaluation, and admission into the next level of care. Some people need both, in that order.
If alcohol, benzodiazepines, head injury, pregnancy, active psychosis, or a seizure history are part of the picture, be more cautious. Those details change where the person can be treated safely.
If you work in caregiving, education, public safety, or any team that may respond to crisis scenes, structured emergency training helps people think clearly under pressure. Resources like ProMed Certifications' ERT course can sharpen response habits that transfer well to behavioral health emergencies too.
What to say on the phone
Long backstories slow things down. Give the facts a nurse, admissions coordinator, or dispatcher needs to place the person correctly.
Use this script:
“I'm with an adult who needs emergency addiction treatment. They used [substance], last used around [time], and they're having [withdrawal symptoms, relapse, overdose reversal, suicidal thoughts, severe intoxication, panic, hallucinations]. Can you do a same-day assessment or admission? If not, where should I take them right now?”
Then add the details that change risk fast:
- alcohol use
- possible fentanyl exposure
- benzodiazepine use
- pregnancy
- seizure history
- head injury
- suicidal statements
- current psychiatric medications
Ask direct questions. Can you medically manage withdrawal here? Do you prescribe medications for opioid or alcohol withdrawal? Do you take people directly tonight, or do they need ER clearance first? If there is no bed, ask where they send people after hours. That question alone can save an hour.
What to have ready before admission
If the scene is safe and the person can tolerate the delay, gather the basics before you leave or call back.
- Substances used: alcohol, fentanyl, heroin, methamphetamine, benzodiazepines, cocaine, prescription pills, or a mix
- Last use: even an estimate helps
- Current symptoms: vomiting, shaking, hallucinations, panic, chest pain, suicidal statements, confusion
- Medical issues: seizures, diabetes, heart problems, pregnancy, past detox complications
- Medications: prescriptions, especially psychiatric meds, pain meds, and any medication for addiction treatment
- Practical items: ID, insurance card, phone charger, emergency contacts, simple clothing
A few logistics points matter here. Bring only what is needed for the first day. Leave valuables at home. If the person may bolt, have one sober adult handle the bag and one handle the conversation.
If you are calling several places, keep a short written log. Facility name, time called, who you spoke with, whether they can take the person, and whether they require ER clearance. In a chaotic night, that list prevents repeat calls and mixed instructions.
If you're in Northern California and need a direct example of what a facility line looks like in practice, some programs offer a 24/7 phone and text admissions line specifically for rapid guidance and placement. In a real crisis, a number you can call immediately matters more than a polished website.
Keep the call calm and specific. You are not asking for a favor. You are trying to place a person in the safest setting available tonight.
The First 24 Hours What to Expect During Admission and Detox
The fear of admission is often worse than admission itself. Families picture a locked unit, punishment, or a cold intake process. Patients picture being judged, stripped of control, and forced to suffer.
Good emergency addiction treatment doesn't work like that. It should feel medical, organized, and steady.

What happens when they arrive
Most rapid admissions start with two tracks happening at once. Staff gather safety information, and they begin calming the body down.
Expect questions about:
- what was used and when
- past withdrawal history
- seizure history
- psychiatric symptoms
- current medications
- allergies
- whether the person wants treatment, is ambivalent, or was pushed to come
Belongings are usually checked. Vitals are taken. A clinician assesses whether the person belongs in that setting or needs a higher medical level of care first.
The first job is stabilization, not a perfect life story.
For opioid use, medications such as buprenorphine may be part of treatment. For alcohol or sedative withdrawal, the medical team may use other medications and monitoring to reduce danger and discomfort. The point of medication-assisted treatment (MAT) is not replacing one problem with another. The point is to reduce withdrawal, lower risk, and make it possible for the person to stay engaged long enough for treatment to start working.
What detox should feel like
Detox is a medical procedure. It should not be framed as a test of character.
A well-run program usually focuses on:
- Safety monitoring: watching for worsening withdrawal, dehydration, confusion, or psychiatric instability
- Symptom relief: reducing nausea, agitation, insomnia, body pain, and cravings as appropriate
- Observation for polysubstance use: fentanyl, alcohol, stimulants, benzodiazepines, and other combinations can change the timeline and risk profile
- Planning the next step early: residential care, outpatient treatment, MAT follow-up, therapy, recovery support
This matters even more now because emergency care has moved beyond a detox-only mindset. Public systems such as New York City's have expanded harm reduction access with fentanyl and xylazine test strips, drug checking at five syringe service programs, and naloxone vending machines in neighborhoods with high overdose death rates, while also linking emergency, inpatient, and outpatient addiction services according to NYC alcohol and drug use services information. In practice, that means the first day should address both immediate withdrawal and the risk of what happens after discharge.
If they say no at first
Families often think one refusal means the window closed. It doesn't.
Structured intervention approaches report 80% to 90% treatment entry success, and among the 15% to 20% who initially refuse, about half reportedly enter care within 1 to 2 weeks, according to the Association of Intervention Specialists on intervention success rates.
That doesn't mean you argue harder. It means you stay organized.
Try this approach:
- Lower the temperature. Drop the lecture.
- Repeat the immediate concern. “I'm worried about your safety tonight.”
- Offer one next step, not ten. “Let's do the assessment.”
- Keep the door open. If they walk out, know who to call again and what the next threshold is for 911.
People in withdrawal, shame, fear, or intoxication often say no before they say yes. A calm, persistent structure works better than emotional force.
Navigating Logistics Insurance, Tricare, and Privacy
Money panic can derail urgent care faster than clinical confusion. Families start asking the wrong question: “Can we afford treatment?” The better immediate question is, “What care can be authorized or arranged tonight, and who can verify it for us right now?”
Many treatment programs can verify benefits directly. Let them do that work while you stay focused on the patient.
Insurance questions to ask immediately
When you call the treatment center or your insurer, keep the list short:
- Is detox covered?
- Is residential treatment covered if detox recommends it?
- Do you require preauthorization, and can that start now?
- Is the facility in network or out of network?
- What deductible, copay, or coinsurance applies?
- Is medication-assisted treatment covered?
- What telehealth or intensive outpatient benefits exist after detox?
If insurance language makes your head spin, a plain-English resource like deciphering mental health insurance options can help you understand the terms you're hearing on those calls.
A useful operational fact sits behind these conversations. In the United States, there are about 14,700 facilities providing substance use treatment services. About 83% offer outpatient care, while only 24% offer residential care and 7% offer inpatient care, and bed availability varies widely by state according to KFF's facility and treatment bed overview. That uneven system is one reason admissions staff matter so much. They know where the openings and bottlenecks are.
Tricare and military families
Military families often hesitate because they expect extra bureaucracy or worry that seeking care will automatically destroy privacy. In practice, the smart move is the same as it is for anyone else. Call the program, say you have Tricare, and ask the admissions team to walk you through eligibility, authorization, and level-of-care options.
Bring the sponsor information, insurance card, and any recent clinical details you have. If there's been prior treatment, recent ER care, or mental health involvement, say that early. It usually speeds up the conversation rather than slowing it down.
What privacy actually means tonight
Families also get stuck on HIPAA. They think privacy rules mean no one can say anything to them.
That's not quite how this feels in real treatment settings. Privacy rules protect the patient's health information, but families can still give information to the treatment team. You can report what substances were used, what you witnessed, past overdose history, suicide concerns, medication details, and what happened leading up to tonight.
Tell staff what you know even if the patient doesn't want to talk yet. Silence helps no one in an emergency.
If the patient signs a release, staff can usually share much more with you. If they don't, you can still pass along critical facts. In the first day, that can make care safer.
From Stabilization to Long-Term Recovery
The most common mistake after emergency addiction treatment is assuming the crisis ended because the person is calmer. A quiet patient in a detox bed is not the finish line. It's the handoff point.
Relapse risk remains high when care stops at stabilization. Relapse rates for substance use disorders commonly fall in the 40% to 60% range, and outcomes improve with longer treatment, often 90+ days, while MAT plus behavioral therapy can produce retention rates up to 70%, according to this review of relapse, treatment length, and MAT retention.
Why discharge is a high-risk moment
Detox clears the body enough for better decisions. It does not rebuild routines, coping skills, housing stability, sleep, relationships, or judgment overnight.
A weak discharge sounds like this:
- “Call around when you get home.”
- “Here's a list.”
- “Try meetings.”
- “Come back if it gets worse.”
A stronger discharge includes actual appointments, medication follow-up, transportation planning, and a named next level of care.
What a real handoff looks like
The better model is simple. Before discharge, the team and patient agree on the next setting and the first contact.
That may mean:
- Residential treatment for people who need structure and separation from triggers
- Intensive outpatient care for people who are stable enough to live at home but need frequent support
- MAT follow-up for opioid or alcohol use disorder
- Telehealth and counseling when geography, work, or family duties make in-person care harder
- Relapse prevention planning with trigger identification, coping tools, and accountability
The emotional shift matters too. Families need to stop chasing promises and start supporting structure. Recovery usually looks less dramatic than the crisis did. It's appointments, medications, sleep, food, boundaries, rides, follow-up, and repeating the plan on ordinary days.
Emergency treatment can still become a turning point. Not because one hard night magically changes everything, but because the right response in that 72-hour window keeps the person alive long enough to enter real care and stay there.
If you need immediate, compassionate help in Northern California, Addiction Resource Center LLC offers medically supervised detox with MAT, residential rehab through its partner Ona Treatment Center, in-person and telehealth IOP, support for co-occurring mental health needs, and a 24/7 phone/text line at 530-625-7910. The team works with adults 18+, families, insured patients, and Tricare beneficiaries who need a clear next step right now.