You may be reading this after another hard night. Maybe you promised yourself this would be the last time. Maybe you're exhausted from hiding it, bargaining with it, or trying to control it on your own. Maybe you're not even sure whether you need detox, rehab, counseling, medication, or just someone to tell you what …
You may be reading this after another hard night. Maybe you promised yourself this would be the last time. Maybe you're exhausted from hiding it, bargaining with it, or trying to control it on your own. Maybe you're not even sure whether you need detox, rehab, counseling, medication, or just someone to tell you what to do next.
Seeking a way to be sober for life means you're already doing something important. You're turning toward help instead of away from it. That matters. It also takes courage, especially when shame, fear, cost, family pressure, or simple logistics have made getting help feel harder than it should be.
You're not the only person facing that wall. In 2024, 48.4 million Americans age 12 and older had a substance use disorder, and only 23% of those who needed treatment received it, according to American Addiction Centers' 2024 addiction statistics summary. The gap isn't proof that people don't want help. It often reflects stigma, confusion, transportation problems, work obligations, childcare needs, insurance issues, and the fear of being judged.
Recovery works best when it becomes practical. Not just emotional. Not just inspirational. Practical means safe withdrawal, the right level of care, repeatable coping skills, a real aftercare plan, and a clear way to pay for treatment without getting lost in paperwork. That's how long-term sobriety becomes real in daily life.
Table of Contents
- Your Journey to Lifelong Sobriety Starts Here
- Taking the First Step Your Safe Start to Sobriety
- Finding Your Fit in a Structured Treatment Program
- Building a Relapse-Proof Life with Essential Skills
- Designing Your Aftercare Blueprint for Long-Term Success
- Navigating the System with Insurance and TRICARE
Your Journey to Lifelong Sobriety Starts Here
Wanting to be sober for life doesn't mean you have to feel certain today. Instead, individuals often feel two things at once. Relief that something has to change, and fear about what that change will require.
That mix is normal. So is ambivalence. A person can be tired of drinking or using and still worry about withdrawal, work, family reactions, privacy, or whether treatment will fit their life. None of that means you're not ready. It means you're human.
Start with one decision, not your whole future
The most useful mindset is simple. Don't try to solve the next ten years tonight. Make the next right decision. Call for an assessment. Tell one safe person the truth. Stop trying to white-knuckle withdrawal alone. Ask what level of care fits your situation.
Recovery isn't built by one heroic promise. It's built by a series of doable choices made close together.
People often get stuck because they think lifelong sobriety means never struggling again. That's not how recovery works in practice. It works when you build enough support, structure, honesty, and follow-through that alcohol or drugs stop being your main answer to stress, pain, boredom, or escape.
What helps early, and what usually doesn't
A few patterns show up again and again in successful recovery.
What helps: getting medically assessed before stopping suddenly, especially if alcohol or sedatives are involved
What helps: choosing a level of care based on need, not pride
What helps: telling the truth about relapse history, mental health, and home triggers
What helps: making finances and insurance part of the plan from the start
What usually doesn't: trying to detox in secret
What usually doesn't: picking the least intensive option just to get it over with
What usually doesn't: assuming motivation alone will carry you through cravings, insomnia, anxiety, and stress
What usually doesn't: treating discharge as the finish line
If you're at the beginning, don't measure yourself by how calm or confident you feel. Measure yourself by whether you're willing to take the next concrete step. That's enough to begin.
Taking the First Step Your Safe Start to Sobriety
The first stretch of sobriety is often the most intimidating because your body and brain are reacting in real time. You may feel shaky, nauseated, panicked, exhausted, restless, sweaty, angry, numb, or all of the above. That doesn't mean you're failing. It means your system is adjusting.

What to do in the first day
If you think withdrawal could be significant, the safest move is to seek a professional assessment immediately. This matters most if alcohol, benzodiazepines, or heavy long-term use is involved. A medical team can evaluate risk, monitor symptoms, and decide whether detox should happen in a supervised setting.
A practical first-day checklist looks like this:
- Call a treatment provider or crisis line: Ask for a same-day substance use assessment.
- Be honest about what and when you used: Leave out as little as possible. Safe treatment depends on accuracy.
- Report past withdrawal problems: Seizures, hallucinations, blackouts, severe anxiety, or prior detox complications matter.
- Mention medical and mental health conditions: Depression, trauma, panic, chronic pain, and medications change the treatment plan.
- Arrange support for logistics: Childcare, pets, work contact, and transportation become easier when handled early.
Practical rule: If stopping on your own feels scary, that's already useful information. Get assessed before trying to push through it alone.
What detox and MAT actually mean
Medical detox means trained clinicians help your body withdraw as safely and comfortably as possible. It isn't a moral test. It isn't about proving toughness. It's a medical process for a medical condition.
Medication-assisted treatment, often shortened to MAT, is another area where people carry a lot of misunderstanding. MAT uses prescribed medications to reduce withdrawal symptoms, curb cravings, or support stability so the person can engage in counseling, groups, sleep, nutrition, and daily functioning. It's a treatment tool, not a shortcut.
Some people need detox first and then step into residential care or outpatient treatment. Others begin with a medical evaluation and move directly into ongoing treatment with medication support. The right path depends on the substance involved, physical risk, mental health needs, and home environment.
What the assessment usually focuses on
An initial assessment typically looks at a few concrete questions:
| Focus area | What clinicians are trying to learn |
|---|---|
| Current use | What substances are involved, how often, and how recently |
| Withdrawal risk | Whether symptoms could become dangerous or severe |
| Mental health | Whether anxiety, depression, trauma, or other conditions need integrated care |
| Home setting | Whether your environment is stable enough for outpatient care |
| Motivation and support | Who can help, what has worked before, and where relapse risk is highest |
People often expect the first step to feel dramatic. More often, it feels structured. You answer questions. You get a recommendation. You stop carrying the whole thing by yourself. That structure is a relief for many people because it replaces panic with a plan.
Finding Your Fit in a Structured Treatment Program
Once withdrawal is addressed, the next question is fit. Not every person needs the same level of care, and choosing well matters. The best program is the one that matches the severity of the problem, the stability of the home environment, the presence of co-occurring mental health needs, and the amount of daily structure required.
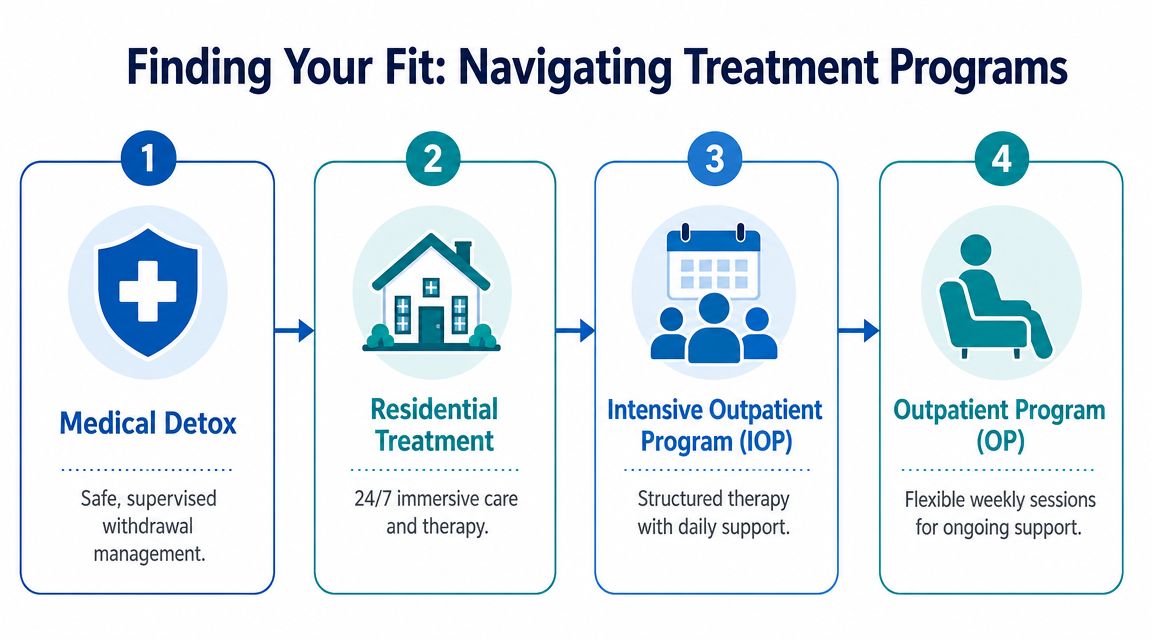
How the main levels of care differ
Some people hear treatment options and think in terms of good versus bad, or serious versus less serious. That's the wrong frame. These are different tools.
| Level of care | Best fit for | Common strength |
|---|---|---|
| Medical detox | People with significant withdrawal risk | Safety and symptom management |
| Residential treatment | People who need distance from triggers and round-the-clock structure | Full immersion in recovery |
| Intensive outpatient program | People who need strong support but can live at home safely | High accountability with daily-life practice |
| Outpatient or telehealth | People with solid stability and lower acuity, or step-down support after higher care | Flexibility and continuity |
A person living in a chaotic household with easy access to substances may do poorly in outpatient care, even with good intentions. A person with a supportive home, reliable transportation, and strong motivation may do very well in an intensive outpatient program while keeping family and work responsibilities in place.
A simple way to choose the right intensity
Ask three plain questions.
First, can you stay physically safe outside of a controlled setting?
Second, can you stay away from the people, places, and patterns that fuel use?
Third, can you engage in treatment consistently without someone else structuring most of your day?
If the answer to those questions is mostly no, higher structure usually makes sense. If the answers are mostly yes, a strong outpatient track may be appropriate.
Duration and structure aren't minor details. In a longitudinal sober living study, abstinence increased from 11% at entry to 68% at 6 and 12 months, and 12-step involvement was the strongest predictor of abstinence for at least 6 months, along with lower substance-use severity and fewer arrests, according to the National Center for Biotechnology Information study on sober living outcomes. In practice, that tells us recovery often improves when people stay in structured environments long enough for gains to stabilize.
People tend to underestimate the middle of recovery. Early progress feels important because it is. But the middle is where routines become durable.
Real-life examples of fit
Consider these side-by-side examples:
- A person leaving detox with strong cravings, unstable housing, and repeated relapses: Residential treatment is often the safer choice because daily triggers are still too close.
- A parent with a stable home, committed family support, and the ability to attend therapy several times a week: An intensive outpatient program may offer enough structure without full separation from home.
- A person stepping down after residential care: Telehealth or outpatient sessions can maintain momentum while re-entry stress rises.
- A person with both substance use and mental health symptoms: Integrated treatment matters more than a one-size-fits-all program label.
The strongest plans usually don't end at one level of care. They move in stages. Detox to residential. Residential to IOP. IOP to outpatient and peer support. That stepped approach gives sobriety somewhere to grow.
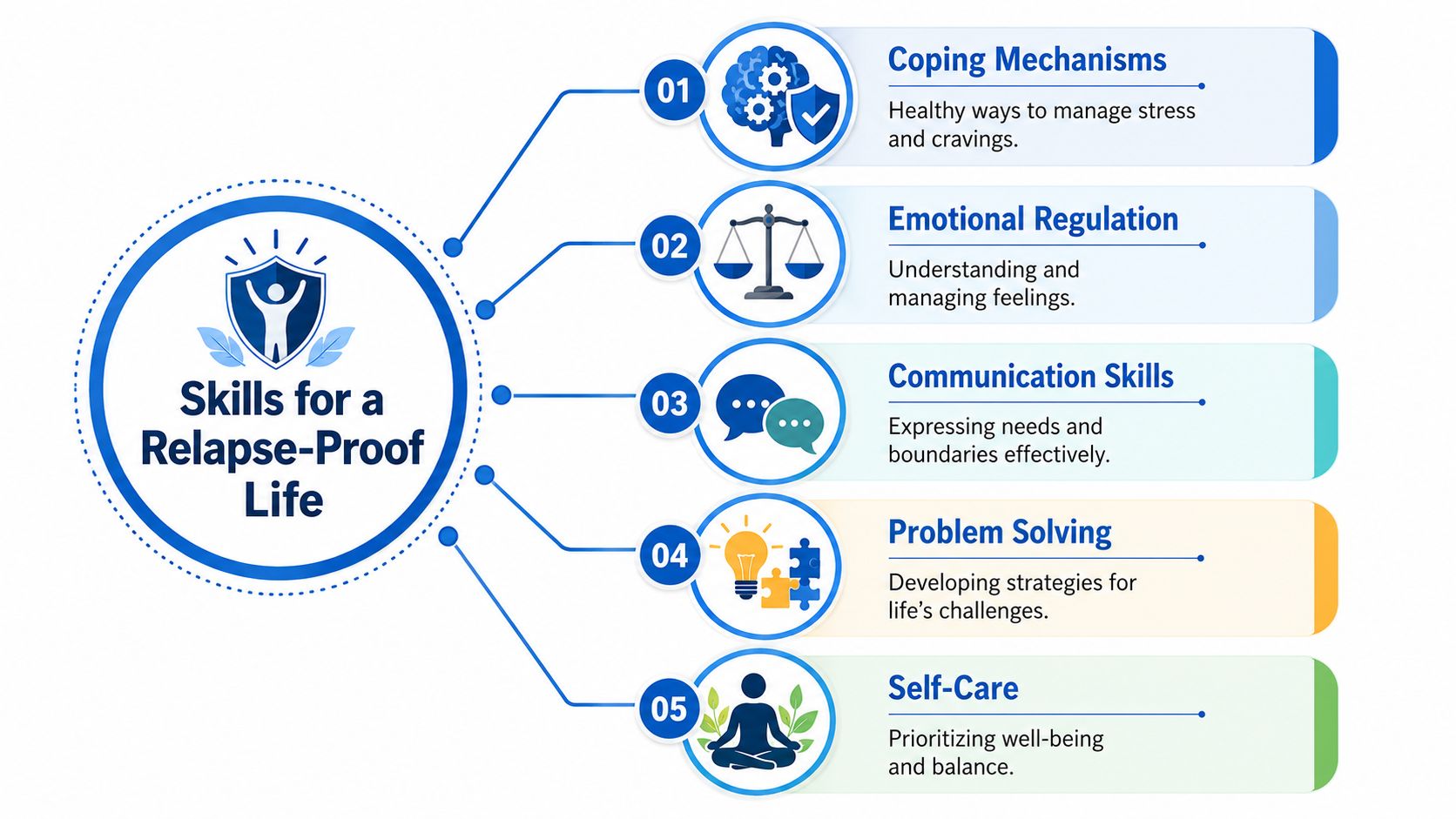
Building a Relapse-Proof Life with Essential Skills
Getting sober and living sober aren't the same task. The first asks you to stop. The second asks you to build. A sober-for-life mindset depends less on sheer willpower and more on daily skills that reduce pressure, interrupt old patterns, and make your life more manageable.
A useful visual can help organize those skills.
Know your triggers before they run the day
A trigger isn't just a bar, a bottle, or a text from an old using friend. Triggers are often internal. Fatigue. Shame. Payday. Loneliness at night. Conflict after work. A certain freeway exit. Unstructured weekends. The thought, "I've been doing well, so maybe I can handle it now."
Write your triggers down in categories:
- People: old using partners, enabling relatives, chaotic relationships
- Places: liquor stores, neighborhoods, houses, events
- Feelings: anger, grief, boredom, anxiety, guilt
- States: hunger, isolation, poor sleep, physical pain
- Thought patterns: minimizing consequences, romanticizing past use, bargaining
Once triggers are named, they become easier to plan for. If Friday evening is dangerous, the answer isn't just "be stronger Friday." The answer is to change Friday.
Build routines that lower pressure
The brain in early recovery doesn't benefit from long stretches of empty time. Structure reduces decision fatigue. It also cuts down the moments where cravings slide in because nothing else is in place.
This short video offers a grounded reminder that recovery skills are lived, not just learned in a session.
A protective routine often includes:
| Time of day | Helpful anchor |
|---|---|
| Morning | Wake time, medication if prescribed, food, hydration, one planned task |
| Midday | Therapy, work, meeting, movement, check-in with support person |
| Evening | Dinner, low-stress activity, meeting or journaling, sleep routine |
You don't need a perfect life schedule. You need repeatable anchors. Small habits matter because relapse often grows in disorganized space.
Practice the skills before you need them
Relapse risk is real, especially early. NIDA-described relapse rates for substance use disorders are typically 40% to 60%, and one synthesis reports that after 5 years of continuous sobriety, relapse risk drops to under 15%, according to Willingway's review of relapse risk and sober living support. The point isn't fear. The point is planning. Recovery gets steadier over time, but the early phase needs active protection.
That protection usually includes a few core skills:
- Craving surfing: Notice the urge, name it, and let it peak without obeying it. Most urges rise and fall.
- Delay and disrupt: Tell yourself you'll revisit the urge after a walk, shower, meal, or call. Don't negotiate while flooded.
- Boundary scripts: "I can't be there." "I'm not drinking." "Don't bring that around me." Simple sentences work.
- Emotional regulation: Breathing skills, grounding, journaling, therapy homework, and movement help reduce the urge to escape.
- Replacement activities: Meetings, volunteering, art, lifting weights, church, hiking, classes, recovery groups, or time with safe people
A craving is not a command. It's a state that passes faster when you stop feeding it secrecy and access.
People trying to be sober for life often make one early mistake. They focus only on avoidance. Avoidance is necessary, but it isn't enough. You also need something to move toward. Purpose, connection, repair, and a life that feels worth protecting.
Designing Your Aftercare Blueprint for Long-Term Success
Many treatment plans are strongest at admission and weakest at discharge. That's backwards. The day structured treatment ends is often when daily temptations, transportation demands, family strain, work stress, and overconfidence all start colliding. Aftercare isn't extra credit. It's the bridge between treatment and ordinary life.

What a strong aftercare plan includes
A good aftercare blueprint is written down. Not vaguely intended. Written. If it only lives in your head, it gets weaker the first time stress spikes.
These are the pieces I most want people to lock in before discharge:
- Meeting schedule: Decide which mutual-help or peer-support meetings you'll attend, on which days, and how you'll get there.
- Therapy continuity: Have the first appointment scheduled before treatment ends, not weeks later.
- Medication follow-up: If you're on MAT or psychiatric medication, know who will manage prescriptions and when.
- Crisis contacts: Keep a short list of people to call before a lapse becomes a full return to use.
- Environment changes: Remove alcohol, drugs, paraphernalia, dealer numbers, and easy access points.
- Daily anchors: Sleep, meals, work or volunteering, movement, and recovery time belong on the calendar.
Some people thrive in 12-step groups. Others connect more with alternatives like SMART Recovery, faith communities, alumni groups, or a combination. What matters is not picking the trendiest support. It matters that you use it.
How family can help without taking over
Families often want to help, but they don't always know how. They may swing between rescuing, policing, withdrawing, or pretending everything is fine. None of those patterns creates steady support.
A healthier family role looks like this:
| Supportive action | Why it helps |
|---|---|
| Clear boundaries | Reduces chaos and mixed messages |
| Family therapy | Gives everyone a place to address trust, anger, and communication |
| Encouragement without surveillance | Supports dignity while staying honest |
| Participation in recovery education | Helps loved ones respond with skill instead of panic |
The family doesn't need to become the treatment program. They need to become consistent.
If you're the person in recovery, tell loved ones exactly what is useful. Rides to meetings. Childcare during therapy. No alcohol in the house. Fewer interrogations. More direct communication. Specific requests work better than hoping people will guess.
The long view matters here. An 8-year study of nearly 1,200 adults with alcohol addiction found that about one-third maintained sobriety in the first year, rising to 50% after the first year and to 85% after 5 years. The same source also notes that 80% of people who try to stop using alcohol relapse at least once before achieving recovery, according to Sprout Health Group's summary of long-term alcohol recovery statistics. That tells me two things. Lasting sobriety is achievable, and setbacks don't erase the larger recovery process.
An aftercare blueprint should reflect that reality. Plan for success, and also plan for vulnerability. If a slip happens, the next move should already be decided. Who do you call. Where do you go. What gets restarted immediately. That's how people protect long-term recovery without turning one mistake into a collapse.
Navigating the System with Insurance and TRICARE
A common recovery moment looks like this. Someone is ready to get help, then stalls out at the kitchen table with an insurance card, a phone in hand, and no idea what to ask. The clinical need is clear. The financial path is not.
I see this often. Cost confusion delays detox, shortens treatment stays, and pushes people to skip therapy, medication follow-up, or outpatient care that would have helped stabilize early recovery. For a sober-for-life plan to hold up, financial access has to be built into the plan from day one.
Start small. Get your insurance card, a notebook, and 20 to 30 quiet minutes. Then call either your insurer or the treatment center's admissions team and ask for a benefits check for substance use treatment. You do not need perfect language. You need usable information.
These are the terms to get clear on:
- Deductible: What you may have to pay before your plan starts sharing more of the cost
- Copay or coinsurance: The portion you pay for visits, services, or treatment
- Out-of-pocket maximum: The most you are expected to pay for covered care during the plan period, based on plan rules
- In-network provider: A facility or clinician contracted with your insurer
- Preauthorization: Approval some plans require before certain services begin
If those terms blur together, a plain-English guide to understanding health insurance plans can help you sort out the basics before you start making calls.
Keep the conversation concrete. Ask the representative to repeat anything unclear. Ask for the person's name, the date, and a reference number for the call. Write down what they say while you are hearing it.
When you speak with a treatment program, ask direct questions that affect both safety and cost:
- Do you accept my exact insurance plan?
- Are you in network or out of network?
- Can you verify my behavioral health and substance use treatment benefits today?
- What levels of care are covered, such as detox, residential, PHP, IOP, or outpatient?
- Do I need preauthorization before admission?
- What will I likely owe upfront, if anything?
- Are medications for addiction treatment covered in the program?
- How are follow-up therapy and telehealth visits billed after discharge?
- What documents do you need from me to start the process now?
- If my coverage is limited, what lower-cost or in-network options do you recommend?
That last question matters. A good admissions team should help you compare options, not just sell a bed. In practice, the best treatment plan is not always the most intensive one on paper. It is the one you can start promptly, afford to continue, and follow through on after discharge.
TRICARE deserves its own attention because families often assume "accepted" means "ready to admit." It can be more involved than that.
For service members, military families, and some beneficiaries, TRICARE can cover substance use treatment well, but the details matter. Plan type affects referrals. Provider status affects whether the care is authorized. Level of care affects what approvals are needed. I tell families to ask a more useful question than "Do you take TRICARE?" Ask, "Are you TRICARE-authorized for my level of care, and what do you need from me today to get approval started?"
That wording saves time.
If you are using TRICARE, have your member information ready, along with a brief treatment history, current substance use concerns, and any recent mental health diagnoses or medications. Ask about the full chain of care, not just admission. Confirm coverage for detox if needed, then ask about residential or outpatient treatment, therapy, psychiatric care, and medication follow-up. Recovery gets shakier when the first week is covered but the next three months are left vague.
Co-occurring mental health needs add another layer to verify. As noted earlier, many people entering treatment need help for both substance use and mental health symptoms. Make sure the program can treat both under your coverage, or explain clearly how care would be split between providers.
Getting help is also a paperwork task. Handling insurance early protects treatment continuity later.
You do not need every billing detail before making the first call. You need enough clarity to keep moving. One answered question at a time is often how families get from fear to admission.
If you or someone you love is ready to take the next step, Addiction Resource Center LLC offers compassionate support for detox, MAT, residential rehab through its partner facility, and in-person or telehealth IOP. Their team works with adults and families, accepts most major insurance plans, welcomes TRICARE beneficiaries, and can help you sort out treatment options without judgment. You can reach Addiction Resource Center in Yuba City at 530-625-7910 for guidance, a confidential conversation, or help starting care.