You may be reading this after a hard night, a frightening relapse, or a long stretch of wondering why sheer willpower hasn't been enough. Maybe you're looking for help for yourself. Maybe you're a spouse, parent, or adult child trying to understand what treatment could look like in real life. Naltrexone for addiction can be …
You may be reading this after a hard night, a frightening relapse, or a long stretch of wondering why sheer willpower hasn't been enough. Maybe you're looking for help for yourself. Maybe you're a spouse, parent, or adult child trying to understand what treatment could look like in real life.
Naltrexone for addiction can be a useful option, but individuals aren't really asking for a chemistry lecture. They want practical answers. Can it help with alcohol? What about opioids? Why do some people start it easily while others can't? Why does it seem surprisingly hard to find, even though it's an established medication?
This guide focuses on those real-world questions so you can make sense of what naltrexone does, where it fits, and what needs to happen before someone starts it safely.
Table of Contents
- What Is Naltrexone and How Can It Help with Addiction
- Understanding the Science Behind Naltrexone
- Choosing Your Naltrexone Path Oral vs Injectable
- Key Steps for a Safe Naltrexone Initiation
- A Realistic Look at Naltrexone Treatment
- Naltrexone vs Buprenorphine and Methadone
- Your Next Steps to Recovery with Addiction Resource Center
What Is Naltrexone and How Can It Help with Addiction
When people feel trapped by drinking or opioid use, they often assume their only options are to keep struggling or to start a treatment they don't fully understand. Naltrexone offers another path. It's a non-opioid medication used in treatment for alcohol use disorder and opioid use disorder, and it has been part of modern addiction care for decades.

Naltrexone became a foundational medication after FDA approval for opioid dependence in 1982 and alcoholism in 1994, according to the COMBINE-era review summary from CEDAR Colorado. In that alcohol-use evidence summary, 100 mg daily for 16 weeks improved percentage of days abstinent from 75.1% to 80.6% and reduced the risk of a heavy-drinking day from 73.1% to 66.2%. The same review also reported about a 15% absolute increase in good clinical outcomes in one naltrexone group (73.7% vs. 58.2%).
What people usually want to know first
Most patients and families don't ask, “What receptor does it bind to?” They ask simpler questions:
- Will it cure addiction? No. It's a tool, not a cure.
- Can it support recovery? Yes, especially when it's part of a broader treatment plan.
- Is it replacing one addiction with another? No. Naltrexone is different from medications that activate opioid receptors.
- Can it help with alcohol and opioids? Yes, but the way it's started and used can look very different depending on the substance.
Bottom line: Naltrexone can help reduce the pull of alcohol and block the rewarding effects of opioids, which can give a person more space to focus on recovery.
What recovery with naltrexone really means
A medication like this doesn't do the emotional work for you. It doesn't repair relationships overnight, erase withdrawal, or remove stress. What it can do is lower one of the biggest barriers to change: the intense reinforcement that keeps people stuck in the cycle.
That matters because when the reward from alcohol or opioids drops, many people can think more clearly about the next step. That next step is usually counseling, structure, follow-up, and relapse-prevention support.
Understanding the Science Behind Naltrexone
Naltrexone works best when you understand one simple idea. It's a blocker, not a substitute.
If opioid receptors are like locks, opioid drugs are keys that open them. Naltrexone is more like a blocker sitting in the lock. It takes up the space, but it doesn't turn the lock and create the rewarding effect people chase. That's why it can reduce the payoff from using.
Why blocking matters
The FDA label describes naltrexone as a pure opioid antagonist, and notes that a standard 50 mg once-daily oral dose produces adequate clinical blockade of parenteral opioids in treatment settings, according to the FDA prescribing information for naltrexone. The same label states that doubling the dose can extend blockade to about 48 hours, and tripling it to about 72 hours.
For opioid use disorder, that blockade is the core mechanism. If a person uses opioids while the blocker is active, the expected reward is blunted or blocked. That can weaken the cycle of reinforcement that keeps opioid use going.
For alcohol use disorder, the explanation is a little less intuitive. Naltrexone doesn't “neutralize” alcohol the way people sometimes imagine. Instead, it reduces the rewarding effects tied to the brain's opioid-related signaling. In practical terms, some people find that drinking becomes less compelling and heavy drinking becomes easier to interrupt.
A short explainer can help here:
Why naltrexone isn't addictive
This is one of the most common points of confusion. People hear “medication for addiction” and assume it must carry its own dependency risk.
That's not how naltrexone works.
The FDA label states that naltrexone does not produce physical or psychological dependence or tolerance to its antagonist effect. Since it blocks receptor activity rather than stimulating it, it doesn't create the kind of drug reward that drives addiction.
Naltrexone doesn't create a high. It occupies the receptor without activating it.
That difference matters for patients who want a non-opioid option. It also matters for families who worry that treatment means “just another drug.” With naltrexone, the medical purpose is to reduce reward and reinforcement, not replace them.
Choosing Your Naltrexone Path Oral vs Injectable
The two main forms are the daily pill and the extended-release injection. Both can be helpful, but they fit different lives, routines, and treatment goals.
SAMHSA says oral naltrexone is taken daily for alcohol use disorder, while the extended-release injectable form is given every four weeks and is approved for both alcohol use disorder and opioid use disorder, as explained in SAMHSA's naltrexone treatment overview.
How the daily pill fits real life
Oral naltrexone gives people flexibility. A person can take it at home, build it into a morning routine, and work with a prescriber to monitor how it's going. Mayo Clinic dosing guidance summarized by SAMHSA-related clinical information commonly lists 50 mg once a day for alcohol use disorder, and opioid treatment often starts lower before increasing if tolerated.
The pill may fit someone who:
- Wants flexibility: Daily dosing can feel easier to adjust around life events and follow-up visits.
- Likes active involvement: Some patients prefer a daily routine because it keeps treatment visible and intentional.
- Is still deciding long-term plans: Starting with a pill can be a practical way to see whether the medication feels like a good fit.
The downside is simple. You have to keep taking it. If someone struggles with consistency, the daily decision can become the weak point.
When the monthly shot makes more sense
The extended-release injection removes that daily decision. For some patients, that's a major advantage. There's less room for missed doses, skipped doses, or “I'll start again tomorrow” thinking.
That option may fit someone who:
- Has trouble remembering medication
- Wants steadier adherence support
- Prefers fewer treatment decisions during a stressful month
- Is already comfortable with regular clinic visits
Here's a side-by-side view:
| Feature | Oral Naltrexone (Pill) | Extended-Release Naltrexone (Vivitrol) |
|---|---|---|
| How often it's used | Daily | Every four weeks |
| Main practical advantage | Flexibility | Fewer day-to-day adherence decisions |
| Main practical challenge | Must remember it every day | Requires clinic administration |
| Best fit for some patients | People who want control and routine | People who want structure and consistency |
Decision tip: The “better” form is usually the one a person is most likely to use consistently within a larger treatment plan.
One more point often gets missed. Naltrexone isn't meant to carry recovery on its own. Major guidance treats it as part of an integrated treatment approach, which includes counseling and behavioral support. The medication can reduce the pull of substance use, but the day-to-day work of recovery still needs structure around it.
Key Steps for a Safe Naltrexone Initiation
For alcohol treatment, starting naltrexone is usually more straightforward than people expect. For opioid treatment, it can be much harder. This is the opioid-starting problem, and it's the most important safety issue to understand.
The opioid-free waiting period
Naltrexone blocks opioid receptors. If a person still has opioids in their body and takes naltrexone too soon, the medication can trigger precipitated withdrawal. That means sudden, severe withdrawal symptoms because the blocker displaces opioid activity at the receptor.
Medical guidance from UAMS and SAMHSA states that patients should be abstinent from short-acting opioids for at least 7 to 10 days before starting naltrexone, and that the waiting period is longer for long-acting opioids such as methadone, as described by UAMS in its patient guidance on naltrexone.
This is not a technical detail. It's the gate that determines whether naltrexone is a realistic option right now.
If someone is still physically dependent on opioids, naltrexone may be appealing in theory but hard to start in practice.
What safe planning usually involves
The most helpful way to think about starting is not “When can I get the prescription?” but “When can I start safely?”
A safe start usually involves:
Honest reporting of recent opioid use
People often minimize or guess. That can be dangerous. The prescriber needs a clear picture of what was used and how recently.A plan for the abstinence window
The waiting period can be physically and emotionally difficult. This is often where people need the most support.Special caution with methadone or other long-acting opioids
These situations often require more planning because the opioid-free period is longer.Monitoring and follow-up
The first dose shouldn't feel rushed. Patients need clear instructions on what to expect and what to do if something feels wrong.
A lot of disappointment around naltrexone comes from poor timing. Someone hears it's a good medication, asks for it quickly, then learns they can't safely start because opioids haven't cleared. That doesn't mean the medication is wrong. It means the sequence matters.
A Realistic Look at Naltrexone Treatment
Naltrexone has real strengths. It also has limits. People do better when they know both.
What it can do well
For alcohol use disorder, oral naltrexone has some of its strongest evidence in patients with moderate-to-severe dependence, and one clinical review reported an absolute improvement of roughly 15 percentage points in good clinical outcomes (73.7% vs 58.2%) versus placebo, according to the clinical review in PMC. That same review notes something important for expectations: naltrexone tends to reduce heavy drinking more reliably than it increases complete abstinence.
That helps explain why some patients say, “It didn't make me never think about alcohol again, but it made the spiral easier to interrupt.” In real life, that can be a meaningful win.
Naltrexone may be especially useful when a person:
- Wants a non-opioid treatment option
- Has already completed opioid withdrawal
- Needs help reducing the reward from alcohol
- Can pair medication with counseling, monitoring, and relapse-prevention work
Why access is still a problem
A frustrating truth is that evidence and access aren't the same thing. Recovery Research highlighted a major implementation gap, noting that only 18% of treatment facilities surveyed by SAMHSA reported any use of naltrexone, as discussed in this Recovery Research summary on prescribing patterns.
That means some people don't run into a medical barrier first. They run into a system barrier. A program may not offer it. A clinician may be less comfortable prescribing it. A facility may focus more heavily on other medications. Families can mistake that for proof that naltrexone “doesn't really work,” when sometimes it isn't being used consistently.
Practical reality: Underuse doesn't automatically mean weak evidence. Sometimes it means the healthcare system hasn't adopted a tool as broadly as it could.
This is why self-advocacy matters. If you're asking about naltrexone for addiction and the answer is vague, it's reasonable to ask follow-up questions. Is the issue medical suitability, or is the program not set up to use it often?
Naltrexone vs Buprenorphine and Methadone
People often compare these medications as if one must be the “best.” That's usually the wrong frame. The better question is which medication matches the person's current physical state, recovery goals, and safety needs.
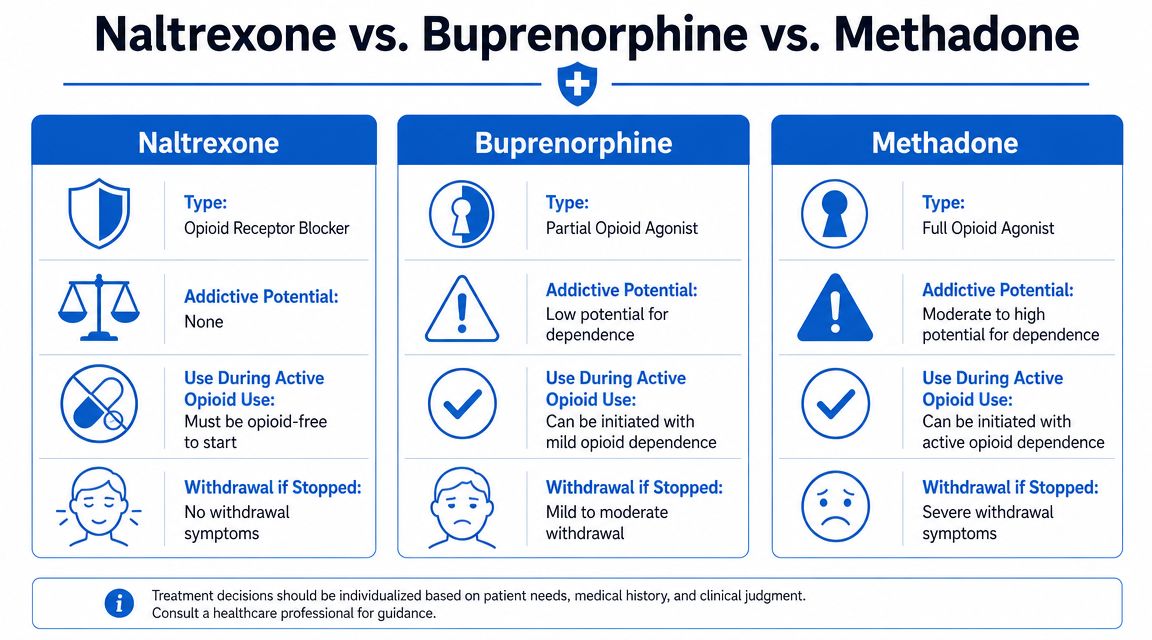
One major difference in plain language
Naltrexone is an antagonist. It blocks opioid receptors.
Buprenorphine and methadone are agonist medications. They activate opioid receptors, though in different ways and to different degrees. That's why they can help people who are still physically dependent on opioids. They address withdrawal and cravings in a way naltrexone does not.
This creates a very different treatment experience:
- Naltrexone: best understood as a blocker and relapse-prevention tool after detox
- Buprenorphine: often used when someone still has opioid dependence and needs help stabilizing
- Methadone: also used for active opioid dependence, often in more structured treatment settings
Who may fit each option
A simple comparison helps:
- Someone fully opioid-free who wants a non-opioid medication may be a reasonable candidate for naltrexone.
- Someone who cannot get through the opioid-free waiting period may be better matched to buprenorphine or methadone.
- Someone with repeated relapse during unstable opioid dependence may need a medication that can be started without fully clearing opioids first.
One reason this comparison matters is that families sometimes hear “naltrexone is non-addictive” and assume it should always be the first choice. But if a person is still actively opioid-dependent, the harder initiation process can make it less practical than buprenorphine or methadone.
The safest medication is often the one a patient can actually start, stay on, and build recovery around.
So the choice isn't moral. It's clinical. Blocking receptors works differently from activating them, and that difference affects timing, comfort, and feasibility.
Your Next Steps to Recovery with Addiction Resource Center
If you're looking at treatment options in Northern California, the most useful next step is a real conversation with a team that understands both the medication and the logistics around it. That matters with naltrexone because the details decide whether a plan is realistic, especially for opioid use disorder where the abstinence period has to be handled safely.
Addiction Resource Center LLC in Yuba City provides a full continuum of care for adults with substance use disorders and co-occurring mental health needs. Services include medically supervised detox with medication-assisted treatment, residential rehabilitation through its partner facility, Ona Treatment Center in Browns Valley, and an Intensive Outpatient Program available both in person and through telehealth.
Their multidisciplinary team includes a medical doctor, registered nurse, licensed counselors, an LMFT, and recovery mentors. That kind of team approach matters because medication is only one part of care. People also need monitoring, counseling, relapse-prevention planning, accountability, and a practical aftercare plan.
If you're trying to sort out pharmacy availability while planning treatment, it may also help to use a patient-friendly tool to find in-stock medications before making multiple calls on your own.
For local families, the logistics are straightforward. Addiction Resource Center LLC is located at 1002 Live Oak Blvd., Suite A, Yuba City, CA. They accept most major insurance plans and welcome TRICARE beneficiaries, which can be especially important for veterans and military families. Their 24/7 phone and text line is 530-625-7910, so you can reach out whether you need help for yourself, guidance for a loved one, or a starting point for detox and outpatient care.
If you're unsure whether naltrexone is the right fit, that's okay. The right first step isn't choosing perfectly on your own. It's getting assessed by people who can help you choose safely.
Addiction Resource Center LLC offers compassionate, down-to-earth support for adults ready to start recovery in Yuba City and across Northern California. If you need detox, medication support, residential rehab coordination, or an in-person or telehealth IOP, their team can help you figure out the next step and begin care quickly.